I received some exciting news today. As always, I am very grateful to everyone who has been supportive of my advocacy and science communication work over the years and who has found it useful (that means all of you!!).
The VIN Veritas Award – from the Latin for truth – honors those who serve science and truth through courage and integrity.
This year, I’m pleased to announce another worthy recipient to join their ranks.
Brennen McKenzie, VMD, MS (Physiology and Behavioral Biology), MS (Epidemiology), is a small animal practitioner, instructor in evidence-based medicine, and author of the Skeptvet blog. Brennen has long been admired by colleagues for his dedication to promoting evidence-based veterinary medicine, and I am delighted that the 2022 VIN Veritas Award judges saw fit to honor his work.
EVIDENCE-BASED MEDICINE There are many characterizations of evidence-based medicine (EBM),1–3 but nearly all include the following core elements:
Explicit integration of controlled research evidence into clinical decision-making
Acknowledgement that some types of evidence are more reliable than others. This is frequently illustrated with hierarchical structures such as evidence pyramids, as in Figure 1.
Recognition that evidence generated by controlled scientific research is generally superior to anecdotal evidence and uncontrolled experience or observation.
A pragmatic acceptance that clinical decisions must be based on the best available evidence, regardless of the level, and should incorporate the judgement of the clinician and the goals and resources of key stakeholders (e.g. human patients or veterinary clients).
Figure 1. Hierarchy of evidence, from most available and least reliable at the bottom to most reliable and least available at the top.4
EBM is a powerful tool for improving patient care, reducing medical errors, compensating for cognitive biases and other sources of faulty decision-making, and meeting the ethical obligations of clinicians to provide the most effective possible treatment and to obtain true informed consent. The major limitations of EBM in veterinary medicine include the paucity of high-quality scientific evidence and a culture of reliance on anecdote and personal experience rather than controlled research evidence.
VETERINARY PALLIATIVE AND HOSPICE CARE The clinical practice guidelines of the International Association of Animal Hospice and Palliative Care (IAAHPC) define palliative care as “relieving or soothing the symptoms of a disease or disorder at any stage of an illness.”5 The American Animal Hospital Association (AAHA) End of Life Guidelines define it as “treatment that supports or improves the quality of life (QOL) for patients and caregivers by relieving suffering.”6 The focus is symptomatic treatment to relieve suffering and improve quality of life, regardless of whether the cause of suffering is a terminal or curable condition. This is, or should be, an integral part of the ordinary practice of veterinary medicine, not relevant only to end of life care.
Hospice, on the other hand, is specific to patients with terminal or incurable conditions, and it is less straightforward to define. According to the AAHA guidelines, it is “philosophy or program of care that addresses the physical, emotional, and social needs of animals in the advanced stages of a progressive, life-limiting illness or disability.”6
The IAAHPC does not provide a single definition, instead discussing the origins and various elements of animal hospice and how it is similar and different from human hospice care. These discussions include the following key concepts:5
Provide palliative care not only for the imminently dying, but also for patients for whom a cure is no longer possible and whose condition has become advanced, progressive, and incurable
Give patients and caregivers control, dignity, and comfort during the time they have remaining to live
Offer spiritual support to patients and accommodates beliefs about death and about afterlife as much as possible. It also provides spiritual and grief support for caregivers
Including hospice-supported natural death as well as euthanasia.
EBM APPLIED TO PALLIATIVE AND HOSPICE CARE Both the AAHA and IAAHPC guidelines, as well as most books and training materials for veterinary professionals dealing with hospice and palliative care, acknowledge the importance of EBM for these disciplines:
AAHA-6
Evidence-based support for specific recommendations has been cited whenever possible and appropriate
Because each case is different, veterinarians must base their decisions and actions on the best available scientific evidence, in conjunction with their own expertise, knowledge, and experience.
Evidence-based research to support this rapidly evolving field is also necessary.
IAAHPC-5
Applying insights and knowledge from bioethics will expedite the development of evidence-based best practices in these emerging fields.
The fields of animal hospice and palliative care are still in the early stages of development and these Guidelines will require revision as evidence-based knowledge advances.
However, organizations and experts in this field also acknowledge that there is a deficiency in the evidence base for many of the practices commonly recommended and employed and that personal experience and extrapolation from human medicine or basic science, both examples of very low-level evidence, form the support for many of the day-to-day interventions and techniques used. This is, of course, also true in most other disciplines within veterinary medicine.
The lack of strong evidence supporting the effectiveness of many practices in hospice and palliative care diminishes the quality of patient care. The history of human and veterinary medicine is rife with ineffective and even actively harmful treatments that were believed to be safe and effective and were widely used for long periods of time before scientific study demonstrated their deficiencies. From bloodletting and homeopathy to thalidomide and internal mammary artery ligation, therapies supported by personal experience and low-quality evidence have been failing patients for thousands of years.7,8
Perhaps a greater challenge to more evidence-based palliative and hospice care than the current lack of high-level evidence is the centrality of philosophical, ethical, and spiritual considerations in these fields. In human hospice, the goals of a hospice program, and the success of hospice and palliative care in any individual case, are inherently intertwined with the beliefs and values of the humans involved. This is an explicit feature of human hospice, where the spiritual beliefs of the human patient and family members are key drivers of the hospice plan for an individual.
Central tenets of the human hospice movement are predicated on contemporary cultural and religious beliefs. For example, a common guiding principle is that hospice care should never hasten death,9 and this is largely a response to general societal views about the sanctity of life and prohibitions on euthanasia, which are rooted in religious and spiritual belief systems.
The animal hospice movement recognizes that veterinary professionals operate in a different context. Our patients cannot express philosophical or spiritual beliefs, and it is debatable whether they are capable of entertaining such beliefs or whether non-human animal cognition encompasses concepts such as the meaning of life or the existence of an “afterlife” of some sort. Euthanasia is also universally legal and widely considered an appropriate choice for animals with impaired quality of life or incurable disease, which provides a very different possible endpoint for hospice care than is usually available for humans.5,6
However, the feelings and belief systems of our patients’ human caregivers are certainly relevant to the formulation and implementation of palliative and hospice care. Philosophical and emotional motivations for choosing natural death rather than euthanasia are likely a significant reason for seeking animal hospice care. The acceptance or rejection of specific treatments is also often informed by such beliefs, which sets limits on the options available to the veterinary team.
EBM is not readily applicable to most religious or ethical issues. When or whether it is acceptable to euthanize an individual animal or permit a natural death, for example, is not a question scientific evidence is well-suited to settle. And while scientific evidence is useful to inform our understanding of how animals experience pain and other forms of physical suffering, it cannot clearly answer existential questions about what meaning life may have to our patients or whether spiritual considerations are relevant to them. The complex ethical balancing of the interests of the patient as understood by the veterinary team and the understanding and interests of the patient’s human family relies more on the domains of ethics and philosophy than on medical scientific research.
Ethical and philosophical issues are relative to one’s particular world view, and this will vary significantly between groups and individuals. Because the community of veterinary professionals actively working in hospice and palliative care is relatively small, the practices and guidelines within the field are heavily influenced by the beliefs and perspectives of a limited number of individuals. This may make the principles and practices of the discipline less compatible with other points of view and could discourage some veterinary professionals or animal owners from providing or seeking palliative and hospice care or taking full advantage of its benefits. As the field grows, a broader range of perspectives may have a beneficial effect on the core principles and common practice.
There are, of course, many aspects of palliative and hospice care to which EBM can and should apply. The safety and efficacy of individual therapies, the most effective way to measure pain and other forms of physical discomfort and to assess the impact of therapies on these, and other important elements of effective palliative and hospice care do depend on accurate knowledge of the kind most effectively generated by controlled scientific research. While there are unique issues in hospice care that influence how we study such questions, there is no doubt that providing effective care requires that the veterinary team and the patients’ caregivers have an accurate understanding of the diseases, symptoms, and treatments involved.
One area that reflects the influence of belief systems and personal experience and the lack of strong EBM standards is the incorporation of so-called complementary and alternative therapies in hospice care. Despite the lack of high-quality evidence for the safety and efficacy of most of these interventions, and strong negative evidence against some, they are widely utilized in both human and animal hospice. Though not mentioned directly in the AAHA guidelines, such alternative practices are explicitly endorsed in the IAAHPC guidelines.5,6
The culture of alternative medicine emphasizes the primacy of personal experience over empirical scientific evidence in evaluating medical treatments, and the role of spiritual considerations in healthcare is often seen as critical.10 These views are also part of the culture of end-of-life care in both human and animal hospice. The training materials for the AAHA certification program in palliative and hospice care explicitly endorse therapies with questionable supporting evidence (e.g. herbal remedies and acupuncture) and those which are clearly only placebos (e.g. homeopathy and “energy” therapies) alongside science-based medical practices. This acceptance of dubious medical practices is likely encouraged by several features of the animal hospice culture and context:
The limited scientific evidence available to assess many common practices
The practical and ethical challenges of conducting high-quality research in patients with terminal conditions
The misperception that the risk of using therapies with inadequate evidence for safety and efficacy are lower in patients with terminal conditions than in patients we hope to cure
The influence of the personal beliefs and experiences of the relatively small number of individuals involved in developing and promoting animal hospice
The culture of the hospice movement, which emphasizes the primacy of individual experiences and beliefs and the centrality of spiritual considerations
TOWARDS MORE EVIDENCE-BASED PALLIATIVE AND HOSPICE CARE High-quality palliative and hospice care for veterinary patients is a critical part of a holistic approach to maximizing animal welfare throughout all life stages. The more evidence-based our treatments and practices are, the more confident we can be that these truly benefit our patients. While scientific research may not always be useful in informing all aspects of end-of-life care, such as supporting the spiritual needs of our clients, it is crucial to ensuring that we understand and meet the physical and behavioral needs of patients. Veterinary professionals and animal owners, like all humans, are easily misled by cognitive biases and placebo effects into inaccurate understandings of nature and the impact of our actions, and EBM can help us avoid such errors and provide the best possible care.11
Steps towards making animal hospice and palliative care more evidence based may include:
Continued recognition of the need for more and better-quality evidence to support palliative and hospice care practices
Improved understanding of the strengths and limitations of different types of evidence and the need to proportion our confidence in specific interventions or beliefs to the strength of the available evidence
Creativity and persistence in the generation of reliable scientific research evidence within the limitations of the palliative and hospice care context
Inclusion of a greater variety of perspectives and world views in establishing guidelines and training for hospice providers to maximize the value of these resources for the broadest possible population of veterinary professionals and animal caregivers
Willingness to change and abandon specific practices based on the best available evidence
REFERENCES
1. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312(7023):71-72. Accessed October 23, 2014. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2349778&tool=pmcentrez&rendertype=abstract
2. Mckenzie B. Evidence-based veterinary medicine: What is it and why does it matter? Equine Vet Educ. 2014;26(9). doi:10.1111/eve.12216
3. Cockroft P, Holmes M. Handbook of Evidence-Based Veterinary Medicine. (Cockcroft PD, Holmes MA, eds.). Blackwell Publishing Ltd; 2003. doi:10.1002/9780470690833
4. McKenzie B. Evidence-based Veterinary Medicine and Personal Bias. In: Ackerman L, ed. Pet-Specific Care for the Veterinary Team. John Wiley & Sons, Inc; 2021:39-42.
5. Shanan, A. August, K. Cooney, K. Hendrix, L. Mader, B. Pierce J. Animal Hospice and Palliative Care Guidelines.; 2009.
6. Bishop G, Cooney K, Cox S, et al. 2016 AAHA/IAAHPC End-of-Life Care Guidelines. J Am Anim Hosp Assoc. 2016;52(6):341-356. doi:10.5326/JAAHA-MS-6637)
7. McKenzie B. Placebos for Pets: The Truth About Alternative Medicine for Animals. Ockham Publishing; 2019.
8. Herrera-Perez D, Haslam A, Crain T, et al. A comprehensive review of randomized clinical trials in three medical journals reveals 396 medical reversals. Elife. 2019;8. doi:10.7554/eLife.45183
9. Finlay I. End-of-life care means exactly what it says: palliative care is about care at the end of life, not about ending life. Futur Healthc J. 2018;5(1):35. doi:10.7861/FUTUREHOSP.5-1-35
10. McKenzie BA. Is complementary and alternative medicine compatible with evidence-based medicine? J Am Vet Med Assoc. 2012;241(4). doi:10.2460/javma.241.4.421
11. McKenzie BA. Veterinary clinical decision-making: cognitive biases, external constraints, and strategies for improvement. J Am Vet Med Assoc. 2014;244(3):271-276. doi:10.2460/javma.244.3.271
INTRODUCTION Experienced clinicians often have an enormous knowledge base about the health problems their patients present with and the available diagnostic and therapeutic options. This knowledge is built over time from a variety of sources: basic pathophysiology and clinical information learned in school; practice tips and pearls imparted by professors and speakers at continuing education meetings; review articles and primary research papers in veterinary journals; textbooks; advice from mentors and colleagues in practice; and, of course, clinical experience with previous cases.
This knowledge base smoothly and efficiently informs the day-to-day activities of clinical practice. When cases with familiar features are seen, the appropriate diagnostic and treatment steps often come to mind automatically, or with minimal prodding. Unlike students and new graduates, experienced clinicians often have little sense of dredging up facts committed to memory and more of a sense of simply knowing things. One of the hallmarks of expertise is that the collating of observations and relevant knowledge into a coherent picture of the problem and a plan become less deliberate and more automatic with time.1
While this process, which is a universal and automatic feature of how the human brain functions, leads to greater efficiency than the explicit, conscious use of algorithms and reference sources employed by less experienced practitioners, it has some serious limitations. One problem, for example, is that the knowledge one relies on often can no longer be connected to its original source. We often simply know things without being aware of how we came to know them. This limits our ability to judge the reliability of the source of our knowledge. In fact, such established, automatic knowing often generates a sense of certainty greater than that which accompanies deliberately seeking and finding information.2 We are more likely to trust what we already know, even if we don’t remember where we learned it, than we are to trust what we have just discovered after searching a trustworthy source of information.
There are also a large number of well-characterized cognitive biases and sources of errors inherent in how our brains acquire, process, store, and utilize information that can lead us astray.3 These are more likely to create error when our reasoning is automatic rather than deliberate, as it necessarily must be in an efficient clinical environment that is not devoted primarily to teaching.
One of the major functions of evidence-based veterinary medicine (EBVM) is to provide tools and resources to make the knowledge base we employ more reliable. This includes generating better quality information through research and facilitating the integration of that information into clinical decision making. When the relevant evidence is of high quality, this can add confidence to our decisions.
More commonly, when the evidence has significant limitations, we may end up with less confidence in our knowledge than we would have without an explicit evaluation of the evidence. However, this is not as undesirable an outcome as it may appear. A clear, accurate understanding of the uncertainty associated with a particular practice protects us, and our patients, from the dangers of acting with unjustified confidence. We are more likely to weigh thoughtfully the risks and benefits of action in the context of an individual case when we understand the degree of uncertainty about our ability to predict or manipulate the patient’s condition.
Being clear about the sources of our knowledge, and the appropriate level of confidence to have in them, also aids in fulfilling our duty to provide clients with informed consent. Surveys of veterinary clients have shown that they value truthfulness highly in the information we provide to them, and that they want to be made aware of the uncertainties involved in the treatment of their animals.4-5 Only if we understand the reliability and limitations of the information we employ in making our recommendations can we give clients the knowledge and guidance they need to make informed choices.
The purpose of these lectures is to examine some widespread or long-standing beliefs and practices in small animal medicine and assess their evidentiary foundations. In some cases, this may clearly validate or invalidate these beliefs. In most cases, however, such an exploration will likely not lead to greater certainty but to a clearer understanding of the degree of uncertainty associated with these beliefs. Hopefully, this will be useful in making clinical decisions and in communicating with clients. The exercise may also be useful in illustrating how to make use of the research literature in establishing and maintaining the knowledge base that informs one’s clinical practice.
Some of the topics that will be covered include:
Metronidazole as a treatment for diarrhea
Tramadol as an oral analgesic
Vitamin C and steroids in sepsis
Common use of gastroprotectants
REFERENCES
Benner, P. From novice to expert. Amer J Nursing, 1982; 82(3):402-7.
Burton, R. On Being Certain: Believing You’re Right Even When You’re Not. New York: St. Martin’s Press. 2008
McKenzie, BA. Veterinary clinical decision-making: cognitive biases, external constraints, and strategies for improvement. J Amer Vet Med Assoc. 2014;244(3):271-276.
Mellanby RJ, Crisp J, De Palma G, et al. Perceptions of veterinarians
and clients to expressions of clinical uncertainty. J Small
Anim Pract 2007;48:26–31.
Stoewen DL, et al. (2014) Qualitative study of the information expectations of clients accessing oncology care at a tertiary referral center for dogs with life-limiting cancer. J Am Vet Med Assoc. 2014;245(7):773-83.
WHAT IS AGING? How we define aging depends on our goals and our frame of reference. From the biomedical perspective of the veterinary clinician, the important elements are:
The passage of time
Deleterious physiologic and functional changes at the molecular, cellular, tissue, and organismal levels
A progressive increase in the risk of the three Ds
Disability
Disease
Death
As cats age, they lose robustness (the ability to maintain a state of baseline or optimal physiologic function in the face of external stressors) and resilience (the ability to return to this state following perturbations caused by such stressors).1 This leads to frailty and the development of many age-associated diseases which seem superficially unrelated but which are actually all consequences of the same underlying mechanisms of aging.2
IS AGING A DISEASE? Because aging is a universal phenomenon, at least in mammals, and because historically there have been no effective interventions to slow or stop the aging process per se, only treatments to mitigate the clinical consequences, aging is widely seen as natural, inevitable, and immutable. However, decades of foundational research in laboratory model species, and more limited recent studies in humans and other species, suggest that the core mechanisms of aging can be altered in a way that may prevent the health consequences of aging. Much debate has focused on the semantic issue of whether or not something natural and ubiquitous but also responsible for illness and death should be labeled a disease.3 There is not yet any consensus resolution to this debate.
A pragmatic approach that avoids this semantic debate is to view aging is the most important modifiable risk factor for disease in companion cats. This is a familiar concept to veterinarians. Obesity, for example, is a risk factor for multiple specific diseases overall mortality hazard.4–6 Focusing on reducing this risk by targeting obesity, rather than waiting for the clinical consequences to develop and then managing each independently is a well-established practice in preventative medicine.
Age-associated changes are responsible for most of the health problems of adult cats, and there are plausible hypotheses suggesting therapies that could directly target aging and so prevent these problems. The focus of geroscience (the study of the fundamental mechanisms of aging) is to identify these targets and therapies so the field of geriatrics (the clinical management of the aged) can move away from the reactive practice of treating the clinical consequences of aging as they arise and towards a preventative approach of delaying and preventing these consequences by modifying the fundamental processes of aging.
HOW DO CATS AGE? The cellular and molecular processes associated with aging, and the tissue dysfunction and ultimate health problems that result from these processes, are complex and multifactorial. Research in laboratory species, and in humans and our feline companions, has elucidated many of these mechanisms, and our understanding of them is growing rapidly. Typical changes include diminished stem cell number and function, declining mitochondrial number and function, accumulation of aberrant and dysfunctional proteins, and many others.7
Despite the complexity of aging, it is ultimately just biology, a collection of physiologic processes that can be understood and manipulated like any other. There is a vibrant field of geroscience research investigating the processes of aging and potential targets for intervention to extend healthspan and lifespan.
Aging manifests in many visible physical changes, from greying and thinning of the coat to lenticular sclerosis and loss of lean body mass. Functional changes include decreased mobility and diminished hearing and vision. Behaviorally, old cats are often less active, less social, and more prone to anxiety and confusion, with many eventually developing cognitive dysfunction.5,8
WHEN IS A CAT “OLD”? A single cutoff for senior or geriatric status is arbitrary and likely to misclassify many cats due to individual variation. Expert guidelines typically consider cats over 10 years of age to be seniors, and this is about the age with mortality appears to begin increasing, at least in some study populations.6,9,10
More important than chronological age, however, is biological age, defined as the degree to which aging has impacted the robustness, resilience, and state of health and function in an individual as measured by physical, functional, and biomarker assessment. We do not yet have reliable tools for measuring biological age, but many are being developed and tested, and ultimately this will be a much more accurate way to predict the age-associated risk of the three Ds (disability, disease, and death) in individual cats.
AGE-ASSOCIATED DISEASES AND CLINICAL PROBLEMS Most categories of disease become more common in older cats, including neoplasia, degenerative musculoskeletal diseases (e.g. osteoarthritis and sarcopenia), chronic kidney disease, and others. Apart from congenital disorders, infections, and trauma, most of the significant diseases and causes of death cats experience result from the progressive accumulation of cellular and tissue changes associated with aging.6,8
Important clinical problems often develop which are not always associated with a specific diagnosis of disease. Loss of mobility, pain, sensory and cognitive decline, and many other such aging changes diminish quality of life, increase caregiver burden, and eventually lead to euthanasia. The common view of these as “natural” and inevitable part of the lifecycle impedes appropriate assessment and management of these conditions and delays necessary research to develop preventative interventions to extend healthspan.
A SYSTEMATIC APPROACH TO THE GERIATRIC FELINE PATIENT Once age-associated health problems do develop, we can best care for our patients with systematic, rational, evidence-based assessment and management. This includes a regular repetition of the following cycle:
Identify important disease and clinical problems
Evaluate these problems using clinical assessment tools
Develop an individualized management plan using available clinical practice guidelines and other scientific evidence
Monitor the progression of the treated conditions and the impact of therapies using clinical assessment tools
Adjust the plan based on follow-up assessment
ASSESSMENT AND MANAGEMENT TOOLS An important part of a systematic approach to geriatric cats is consistent, objective assessment and management of age-related diseases and clinical problems. This is best accomplished with the regular use of validated clinical metrology instruments and reliance, when possible, on evidence-based clinical practice guidelines. There are many CMIs available or in development to quantify pain, quality of life, and the burden of care on the owners of geriatric cats.11–15 Repeated use of these allows detection of changes over time, better evaluation of the effectiveness of therapies than unaided observation, and better communication with owners to facilitate decision making.
There are also numerous clinical practice guidelines available to support management of the most common age-associated problems and diseases.10,16–19 While some are more rigorous and evidence-based than others, all offer rational and systematic approaches that can help clinicians make comprehensive treatment and management plans.
PITFALLS IN FELINE GERIATRICS A systematic approach to geriatric medicine encourages proactive identification of disease and clinical problems and using the best available evidence to guide diagnostic and treatment interventions. Too often, clinical signs of frailty and disease are dismissed as “just slowing down” or “normal aging” rather than appropriately assessed, monitored, and managed. In the future, proactive and systematic detection of such signs will be a critical element in the determination of biological age and the decision to employ therapies targeting aging directly.
REFERENCES
1. Ukraintseva S, Yashin AI, Arbeev KG. Resilience Versus Robustness in Aging. Journals Gerontol Ser A. 2016;71(11):1533-1534. doi:10.1093/GERONA/GLW083
2. Miele A, Sordo L, Gunn-Moore DA. Feline Aging: Promoting Physiologic and Emotional Well-Being. Vet Clin North Am Small Anim Pract. 2020;50(4):719-748. doi:10.1016/J.CVSM.2020.03.004
3. McKenzie BA. Is Aging a Disease? DVM360. 2022;53(3):25.
4. Teng KT, Mcgreevy PD, Toribio JALML, Raubenheimer D, Kendall K, Dhand NK. Associations of body condition score with health conditions related to overweight and obesity in cats. J Small Anim Pract. Published online 2018. doi:10.1111/JSAP.12905
5. Miele A, Sordo L, Gunn-Moore DA. Feline Aging: Promoting Physiologic and Emotional Well-Being. Vet Clin North Am Small Anim Pract. 2020;50(4):719-748. doi:10.1016/J.CVSM.2020.03.004
6. O’Neill DG, Church DB, McGreevy PD, Thomson PC, Brodbelt DC. Longevity and mortality of cats attending primary care veterinary practices in England. J Feline Med Surg. 2015;17(2):125-133. doi:10.1177/1098612X14536176
7. McKenzie BA. Comparative veterinary geroscience: mechanism of molecular, cellular, and tissue aging in humans, laboratory animal models, and companion dogs and cats. Am J Vet Res. 2022;83(6). doi:10.2460/AJVR.22.02.0027
8. Bellows J, Center S, Daristotle L, et al. Evaluating aging in cats: How to determine what is healthy and what is disease. J Feline Med Surg. 2016;18(7):551-570. doi:10.1177/1098612X16649525
9. Quimby J, Gowland S, Carney HC, DePorter T, Plummer P, Westropp J. 2021 AAHA/AAFP Feline Life Stage Guidelines. J Feline Med Surg. 2021;23(3):211-233. doi:10.1177/1098612X21993657
10. Ray M, Carney HC, Boynton B, et al. 2021 AAFP Feline Senior Care Guidelines. J Feline Med Surg. 2021;23(7):613-638. doi:10.1177/1098612X211021538/ASSET/IMAGES/LARGE/10.1177_1098612X211021538-IMG1.JPEG
11. Buffington T. Development and Initial Validation of a Frailty Scale for Domestic cats.
12. Doit H, Dean RS, Duz M, Brennan ML. A systematic review of the quality of life assessment tools for cats in the published literature. Vet J. 2021;272:105658. doi:10.1016/J.TVJL.2021.105658
13. Reid J, Scott EM, Calvo G, Nolan AM. Definitive Glasgow acute pain scale for cats: validation and intervention level. Vet Rec. 2017;180(18):449-449. doi:10.1136/VR.104208
14. Klinck MP, Gruen ME, del Castillo JRE, et al. Development and preliminary validity and reliability of the montreal instrument for cat arthritis testing, for use by caretaker/owner, MI-CAT(C), via a randomised clinical trial. Appl Anim Behav Sci. 2018;200:96-105. doi:10.1016/J.APPLANIM.2017.11.013
15. Spitznagel MB, Jacobson DM, Cox MD, Carlson MD. Caregiver burden in owners of a sick companion animal: A cross-sectional observational study. Vet Rec. 2017;181(12). doi:10.1136/vr.104295
16. (IRIS) IRIS. Treatment Recommendations for CKD in Cats (2019) Treatment recommendations for Cats with Chronic Kidney Disease Stage 1 Feline patients. Published online 2019.
17. Epstein ME, Rodan I, Griffenhagen G, et al. 2015 AAHA/AAFP Pain Management Guidelines for Dogs and Cats. J Feline Med Surg. 2015;17(3):251-272. doi:10.1177/1098612X15572062
18. Sparkes A, Heiene R, Lascelles B, et al. ISFM and AAFP consensus guidelines: long-term use of NSAIDs in cats. J Feline Med Surg. 2010;12(7). doi:10.1016/J.JFMS.2010.05.004
Aging is not an inevitable and immutable fact of life. It is a modifiable risk factor for the most causes of disability, disease, and death in adult cats.
Numerous physical, function, behavioral, and metabolic changes occur in aging cats that lead to clinical disease, frailty, diminished quality of life, and a significant caregiver burden on owners.
Aging is just biology! The cellular, molecular, and tissue changes that occur, and that lead to the feline aging phenotype, are complex but comprehensible. The better we understand these changes, the better we can intervene to mitigate them.
A systematic, evidence-based approach to assessment and management of diseases and clinical problems in geriatric cats, supported by validated clinical metrology instruments and clinical practice guidelines, is a more efficient, comprehensive, and effective strategy for high-quality patient care.
I have put a lot of effort over the last 14 years into investigating questionable remedies for pets, and exposing people who peddle misinformation and snake oil. Pet owners care deeply for their animal companions, and this love can be taken advantage by unscrupulous or deluded individuals who sell untested, unsafe, and ineffective products for sick pets.
My main hope is always that the truth about these products and these individuals will protect some people and their pets from being misled and harmed. In the perfect world, revealing the truth about misinformation and deception might help remove some products and their promoters from the field and discourage some of the selling of snake oil and pseudoscience.
The reality, though, is that there is little effective oversight of healthcare products and services for veterinary patients. Veterinarians and others are generally free to offer practices and products that haven’t been appropriately tested for safety or that are unquestionably ineffective, even dangerous. Regulatory agencies, such as state veterinary medical boards, the FDA, and others, lack the resources and political support to challenge veterinary quackery. The laws are often inadequate to bar specific products or their promoters or obtain justice of compensation for those hurt by bogus treatments.
Gloria Dodd, Al Plechner, Jean Dodds, Karen Becker, and many others are able to freely promote products and practices ranging from the unlikely to the completely insane with little interference. Ineffective and unsafe remedies, from homeopathy to Neoplasene, coffee enemas to untested herbal remedies remain available for use by vets and pet owners regardless of the evidence against them. All too often, no one is truly protecting the public from pseudoscience and quackery.
Today, though, I get to report on one small break in this depressing pattern. Jonathan Nyce, who sold a million dollars worth of his fake cancer treatments, Tumexal and Naturasone, has been convicted of wire fraud and trafficking in illegal veterinary drugs. I first wrote about Tumexal in 2014, and my conclusion then was this:
TumexalTM is yet another purported wonder drug with a “secret ingredient” that has been discovered by a lone genius and offered to the public out of altruism. It is supposed to be very effective and perfectly safe, and anyone who doesn’t take the company’s word for this is a “cynic” with questionable motives or a lack of compassion. Such claims are cheap and easy to make, but they are worthless without real scientific data, and none are available for TumexalTM.
Later that year, the FDA issued a warning to Nyce to stop making illegal claims about the product. Despite this, his web site remained active until 2018, and he was able to continue to take advantage of desperate pet owners and sell his worthless snake oil. Finally, in 2020, the U.S. Attorney for the Eastern District of Pennsylvania charged him with illegal claims and selling misbranded animal drugs. Now, almost three years later, and many, many years after Nyce started selling his snake oil, he has finally been convicted of these charges.
What price Nyce will pay, or what compensation, if any, the pet owners he defrauded will receive is unclear. Much as I would like to take some small comfort in this conviction, I cannot help be frustrated by the slow and ineffective enforcement of even the most minimal protections for pet owners and veterinary patients. Despite a dodgy history in the pharmaceutical industry and being a convicted murder, Nyce was able to sell a fake cancer cure to over 900 pet owners for hundreds of thousands of dollars over at least 6 years without impediment.
When even such an extreme case draws an arguably insufficient response, less dramatic and sensational purveyors of snake oil are likely to be free to mislead the pet-owning public indefinitely. The risk is real, and it is past time we, as a society, got serious about protecting vulnerable animals and their human families.
While the focus of my professional attention, and my writing, has largely shifted away from complementary and alternative veterinary medicine (CAVM) per se and towards the field of aging, I obviously cannot escape the pseudoscience and sloppy or motivated reasoning that characterizes so much of alternative medicine as it pops up often in the aging biology domain as well. Aging is both a legitimate area of scientific inquiry and fertile ground for the growth of snake oil remedies. From the plausible but unproven to the outright ridiculous, purported “anti-aging” products abound, for humans and for our pets.
I’ve already written about the use and misuse of aging science to justify alternative practices in my review of The Forever Dog, where the framework of aging is used to try and give a shiny new luster to so many tired tropes and arguments from the world of CAVM. While attending the recent VMX veterinary continuing education conference in Orlando, I saw the usual profusion of dubious practices on sale, from the traditional nonsense of the Chi Institute’s ‘Traditional” Chinese Medicine training to cold laser devices and, of course, SUPPLEMENTS!!
What’s not to love about a dietary supplement? Virtually no regulation makes creating a new product orders of magnitude cheaper than developing a drug because there is no need to prove it works or is safe. And despite the lack of meaningful evidence for the vast majority of supplements on the market, vets and pet owners just assume they are safe and are willing to use them based on even the thinnest thread of hope that they might do something useful. Billions of dollars to be made with just a little creative marketing and negligible effort or expense for research.
And, of course, aging is a prime target for such supplements since we do not yet have properly validated medicines to target the underlying mechanisms that lead to age-associated disease. I believe such medicines are coming, but the work of development and testing is a lot slower and more challenging that simply extrapolating from some mouse studies and slapping a shiny label and the Quack Miranda Warning on a bottle of some dietary supplement, so it’s a hard temptation for many companies to resist.
While there have been veterinary supplements on the market claiming to target aging in pets for a while, the latest and most visible player in the Expo Hall at VMX was Leap Years from a company called Animal Biosciences.
What is It? Animal Bioscience is a company founded by David Sinclair, his brother Nick Sinclair, and Virginia Rentko, a veterinary internist and researcher. I have written about Dr. Sinclair previously, reviewing his book, Lifespan. He is that fascinating and frustrating, but all too common, chimera- a talented scientist who produces legitimate and valuable research evidence and also a slick salesman who regularly promotes dubious or even clearly false ideas and products. He is particularly famous in the aging biology field for his research, and his business activities, in the area of sirtuins and resveratrol. I have written about resveratrol regularly since 2009, and it nicely illustrates the dangers and pitfalls of excessive hype, enthusiasm, and commercial products based on preliminary preclinical research.
Despite this controversy, Dr. Sinclair is still a prominent advocate for the dietary supplement approach to aging, and he focuses a lot of his attention now on compounds intended to boost NAD+, a ubiquitous and important element in multiple physiologic processes, including many related to aging. Dr. Sinclair has acknowledged taking one of these compounds, NMN, and recommending it to family and friends.
He is also involved in a company, Metro Biotech, that has produced a proprietary version of NMN. This company has been associated with some controversy recently when the FDA banned the sale of NMN supplements. The agency determined that NMN can no longer be classified as a dietary supplement because it is in the process of being evaluated as a possible drug through clinical studies overseen by the FDA. Some have made the claim that Metro Biotech is pursuing a strategy of using the FDA regulatory system to exclude forms of NMN other than its own from the marketplace, though this is only speculation.
In any case, Dr. Sinclair is listed as the founder of Animal Biosciences. The sole product of this company is a supplement called Leap Years. The company does not identify the specific compounds in its product, but one is claimed“ to restore cellular health by boosting NAD+ production,” and it is not much of a “leap” to suspect that the NAD booster they are using is NMN, or even the proprietary version of NMN made by Metro Biotech.
The other ingredient is also not disclosed but is claimed to be a senolytic. These are compounds intended to help with the removal of senescent cells, that is cells with abnormal replication and function that can promote age-related disease through increasing inflammation and other mechanisms. Popular examples include quercetin and fisetin.
The Claims Animal Biosciences makes a lot of claims for their product on their web site and in the materials they provided at the VMX conference. These include-
“clinically proven”
“slows the effects of aging”
“extends the health and vitality of dogs”
Promotes healthy aging
Increased or improved
Cardiovascular function
Circulation
Joint flexibility
Brain health
Cognitive function
More
Vitality
Engagement
Life
The Evidence The support offered for these claims includes reference to “molecules that have proven efficacy in humans,” reference to lab animal studies, and reference to a clinical trial conduction at NCSU veterinary school.
Since there are no proven medications or supplements that extend lifespan and healthspan in humans, the first claim is unsupported. Dr. Sinclair often makes such claims and then references pre-clinical or pilot studies in lab animals and humans, but this is a classic leap beyond the true probative value of these kinds of evidence that supplement manufacturers often rely on. Promising studies suggesting benefits based on basic mechanisms or animal model studies are useful for guiding us towards the most promising targets for real-world clinical trials, but they don’t make these trials unnecessary. Without real-world clinical trial evidence, claims of “proven” efficacy are unjustified.
Similarly, many things have been shown to extend lifespan in rodents and in a few other model species, but the devil is always in the details. Some interventions may work in some strains of mice but not others, in males or females but not both, or they may appear to work for one research group only to be unreplicable by other scientists, as was the case with some of Dr. Sinclair’s work with sirtuins and resveratrol. While the concepts of NAD+ boosters and senolytics are valid, and there is data supporting the potential of some specific agents, we do not have clinical trial evidence showing real-world benefits for this supplement or its ingredients in pet dogs.
Which brings us to the clinical study at NCSU. This study is still enrolling subjects, and no results have been published. Despite this, the company cites the work as evidence its product is “clinically proven,” which is inaccurate and unethical. Once the full results and methods are published, we will have a better sense of the strengths and limitations of this piece of evidence. Even if the results are encouraging, though, more will be needed to build a confident, reliable case that this product will make a real difference in dogs’ lives.
From the perspective of the basic science behind NAD+ boosters and senolytics, the existing evidence is encouraging but by no means definitive. NAD+ levels do decline with age, and this is associated with many negative health impacts that occur during aging. However, there is no consensus that NAD+ precursors or boosters are effective at slowing aging or reducing the risk of age-associated health problems, by raising NAD+ levels or by any other mechanism. Several companies sell NAD+ precursors for dogs, including NMN. None have been demonstrated safe and effective by high-quality clinical studies in dogs (or in humans).
Clearance of senescent cells using senolytic drugs is another popular area of geroscience research, and there are a number of compounds that have been investigated. Other companies also sell supplements claiming they are senolytics that will extend lifespan and healthspan in dogs (e.g. Fisetin Vet). However, as with NAD+ precursors, none of these compounds have been proven effective for this use in human or in dogs with reliable scientific evidence.
Bottom Line Leap Years is similar to most veterinary supplements on the market: It is based on some plausible ideas with limited supporting evidence, and it is marketed with claims that go well beyond anything scientifically proven or reasonable. The potential risk are as uncertain as the potential benefits. While NMN and various senolytics commonly available as supplements have not shown obvious signs of causing health risks, the limited real-world evidence doesn’t allow us to say with confidence that don’t do harm, only that we haven’t found any yet.
As always, using a product with weak evidence for both safety and benefits intended to treat a broad variety of health problems in normal dogs who are currently healthy is a roll of the dice, and the potential outcome is hard to predict. If evidence emerges this specific product truly extends healthspan and lifespan in dogs, I will be first in line to recommend it, but that evidence will need to be a good bit stronger than it is right now.
As you may have noticed, my productivity in writing blog posts has declined significantly this year. A large part of the reason is that I have been spending my time writing scientific publications and preparing continuing education talks for veterinary conferences, all on subjects related to canine aging.
This post is intended to highlight the scientific articles I have written or worked on this year. Hopefully, this will be an interesting introduction to the field of canine aging and the potential for legitimate scientific interventions which can be shown to meaningfully impact aging and the negative health outcomes associated with it.
Currently, most of the advice pet owners receive about aging is unproven or pseudoscientific and unlikely to truly improve the welfare of their pets. Real science is often more nuanced and complex and less sexy and satisfying than pseudoscience due to the frustrating limits set by fidelity to actual scientific evidence. Still, the field of geroscience is a an exciting point where there is the potential to begin translating decades of lab research into clinically useful therapies. As always, we must proportion our confidence (and excitement) to the level of evidence, and we have a long way to go before we can confidently say that Drug X or Practice y will extend your dog’s health span or lifespan. But there is a path forward to doing this, and these articles are my small part in helping to pave that path.
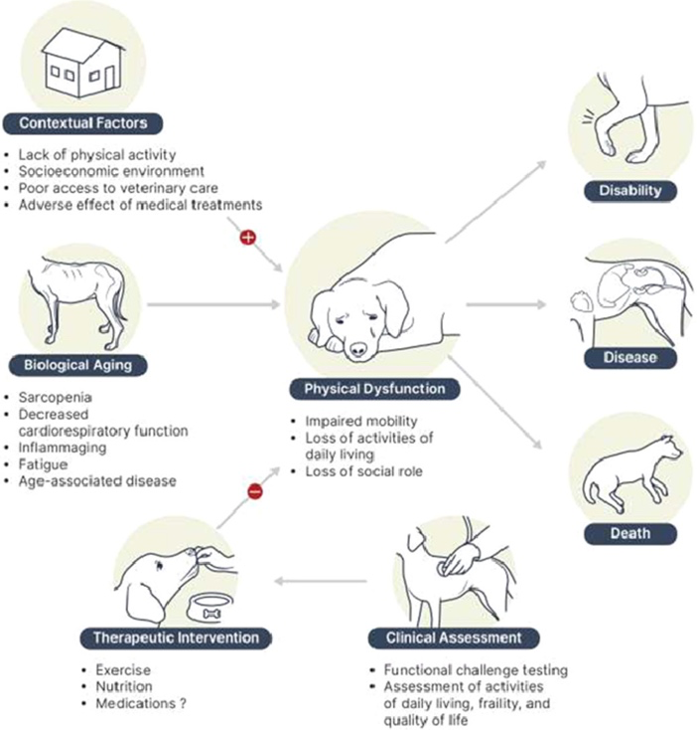
Aging is the leading cause of disability, disease, and death in adult dogs. One major consequence of aging is diminishing physical function. In humans, there are validated clinical assessments of physical function that can predict disability, morbidity, and mortality. There are also effective interventions to preserve and restore function and reduce the risk of death and disease in the elderly. This review evaluates the decline in physical function with age in dogs and the potential utility in this species of clinical assessment tools and interventions developed for humans.
Contrary to the common view of aging as a mysterious and inevitable natural event, it is more usefully understood as a set of complex but comprehensible biological processes that are highly conserved across species. Although the expression of these processes is variable, there are consistent patterns both within and between species. The purpose of this review is to describe the patterns currently recognized in the physical and behavioral manifestations of aging in the dog and how these impact the health and welfare of companion dogs and their human caregivers. This will set the context for future efforts to develop clinical assessments and treatments to mitigate the negative impact of aging on dogs and humans.
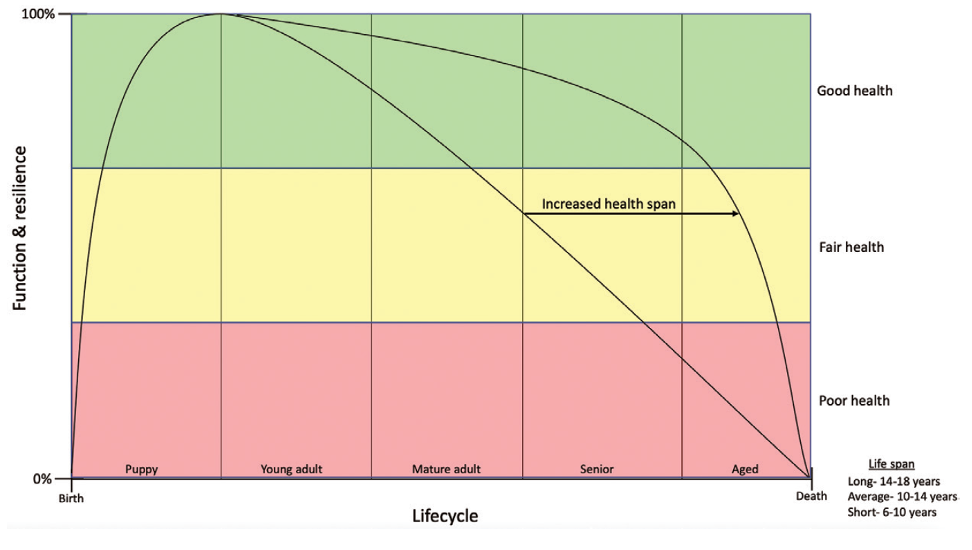
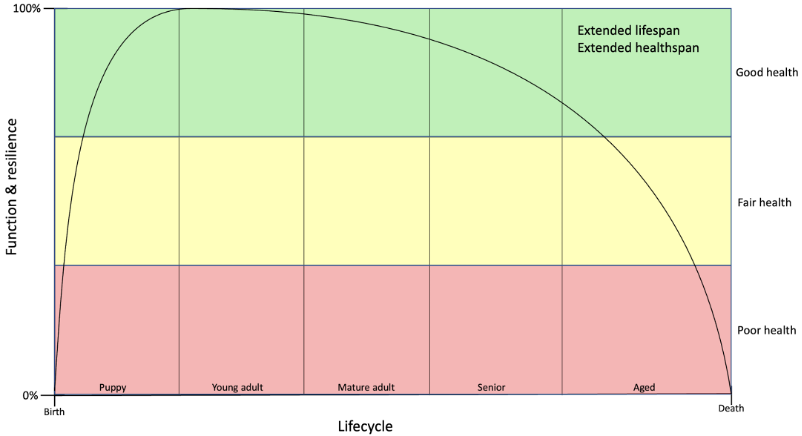
Life cycle trajectories with varying healthspan in dogs. Anti-aging therapies can increase life span (years lived) and healthspan (years lived in good health) by delaying the onset of age-associated disease and disability.
The purpose of this review is to describe key mechanisms of aging at the cellular and molecular level and the manifestations of these in the tissues of the musculoskeletal system, adipose, and the brain. This will highlight knowledge gaps and important targets for future research to extend lifespan and healthspan in dogs and cats.
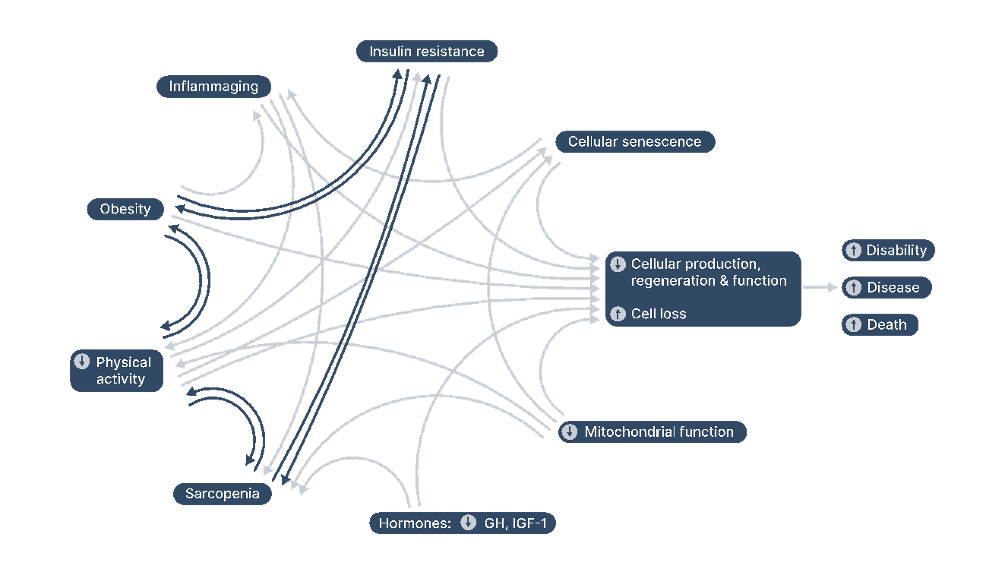
The web of tissue aging—a partial illustration of the interactions between key tissue-aging mechanisms.GH = Growth hormone. IGF-1 = Insulin-like growth factor-1.
In this paper we propose a new conceptual framework for aging in dogs, the Canine Geriatric Syndrome (CGS). CGS consists of the multiple, interrelated physical, functional, behavioral, and metabolic changes that characterize canine aging as well as the resulting clinical manifestations, including frailty, diminished quality of life, and age-associated disease. We also identify potential key components of a CGS assessment tool, a clinical instrument that would enable veterinarians to diagnose CGS and would facilitate the development and testing of interventions to prolong healthspan and lifespan in dogs by directly targeting the biological mechanisms of aging.
Core elements of Canine Geriatric Syndrome and next steps for developing a CGS clinical assessment.
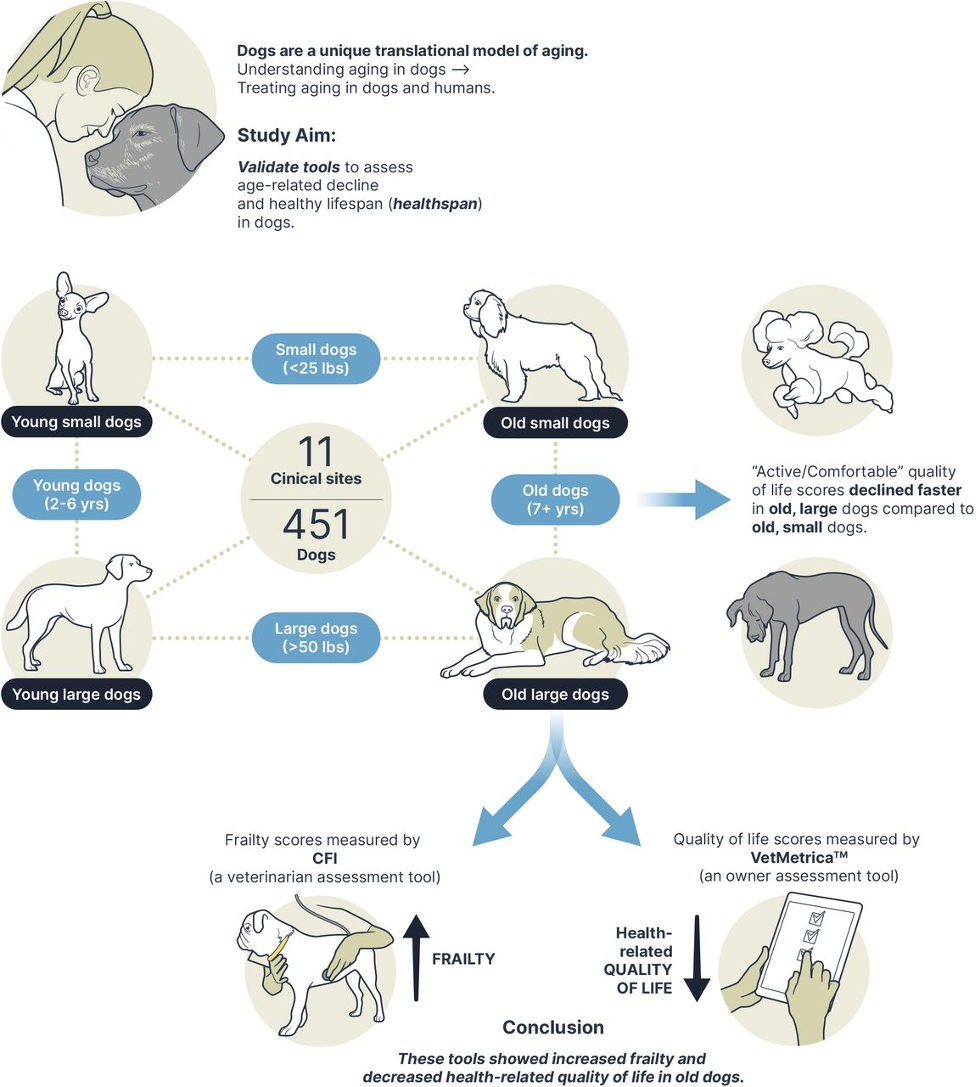
Developing valid tools that assess key determinants of canine healthspan such as frailty and health-related quality of life (HRQL) is essential to characterizing and understanding aging in dogs. Additionally, because the companion dog is an excellent translational model for humans, such tools can be applied to evaluate gerotherapeutics and investigate mechanisms underlying longevity in both dogs and humans. In this study, we investigated the use of a clinical questionnaire (Canine Frailty Index; CFI; Banzato et al., 2019) to assess frailty and an owner assessment tool (VetMetrica HRQL) to evaluate HRQL in adult companion dogs.
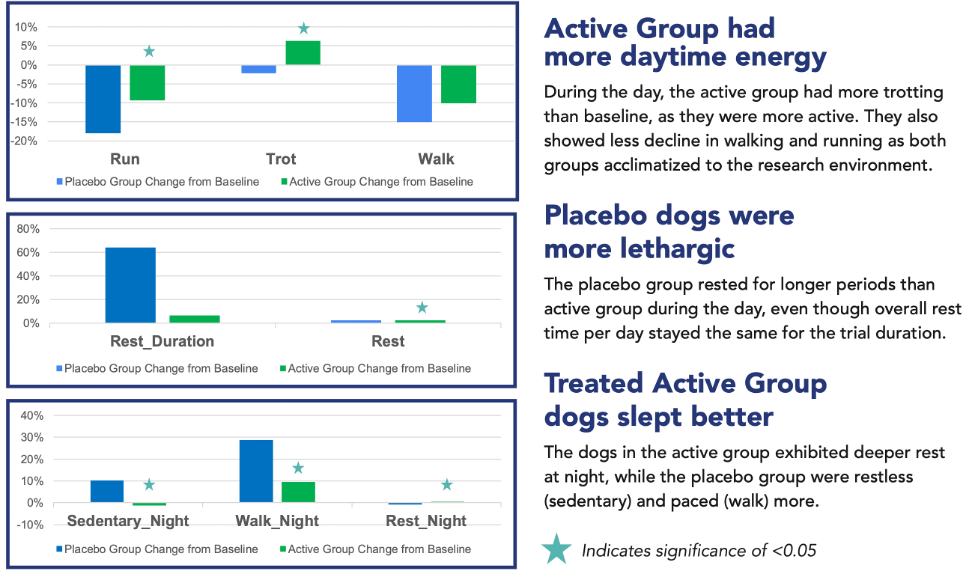
A graphical summary of the Healthspan Study and key results.
This is my last piece for Veterinary Practice News as the EBVM columnist. I chose to focus on the open veterinary hospital model, which I have been a proponent of for many years.
There is widespread recognition in veterinary medicine of the critical role clients and client communication play in patient care. Informed consent and establishing a veterinarian-client-patient relationship (VCPR) are typically legal prerequisites for providing veterinary services. On a more pragmatic level, we cannot care for our patients effectively without the understanding and engagement of their owners, as well as their consent.
Many strategies have been investigated and promoted to improve client communication,1,2 generally with the aim of improving acceptance of veterinary recommendations. In addition to specific communication strategies, establishing an effective VCPR requires building rapport and trust between pet owners and veterinarians. This is especially true for managing complex, ongoing medical problems.
One approach I have experienced and believe deserves greater study and broader adoption, is the open-hospital model.3For most of my career, I have worked in a hospital that encourages clients to be with their pet at any time while they are in our care, whether in the exam room for a routine checkup, hospitalized in the ICU, and even during dentistry, surgery, or other invasive procedures.
Some are horrified
I am no longer surprised, albeit still amused, by the horror that many of my colleagues display when I tell them about our open-hospital policy. The idea of drawing blood or vaccinating a patient with the owner present, much less allowing them to observe us performing surgery, is sometimes seen as dangerous, if not completely insane.
When exploring this response, the justifications for the horror usually involve concerns about negative client reactions, from fainting at the sight of blood to misperceiving restraint or invasive procedures as abuse and deciding to sue. Veterinarians and veterinary nurses also worry their own anxiety about being watched by owners will degrade their performance, particularly for technical procedures. Legal liability for owner injury is also a common concern.
All of these issues are, of course, real potential negative consequences of having clients accompany their pets through all stages of veterinary care. My own experience, however, suggests these are rare outcomes that are more than balanced by the benefits of an open-hospital model. Appropriate policies and safeguards can minimize the risks and maximize the benefits of this approach.
The benefits pertain to both owners and patients. There is some evidence that dogs, for example, are more relaxed and compliant during veterinary treatment when their owners are present.4,5 The fact our patients, a social species with close relationships to individual humans, should take comfort in the presence of their human caregivers is not surprising. Certainly, we take such comfort from the presence of family members when we receive medical care.
Our clients also benefit from being able to be present for all aspects of their pets’ care. This enhances their trust and confidence in our treatment of their pets by taking away the uncomfortable sense we are doing scary and painful things to their companions “in the back.” Clients can see how much we care for our patients, how we try to comfort them, and treat them well, even when they are fractious. It is also often easier to explain the nature of a health problem when the client can see the images or the lesions directly. Being a part of the process makes clients feel more like the partners they should be in the medical care given to their pets, and it helps build familiarity and relationships between clients and the veterinary team.
There are benefits to veterinary professionals, as well, from having clients accompany their pets in the hospital. Watching the veterinary team provide care illustrates the difficulty and complexity of what we do, and helps show how much skill is required and why we are justified in charging appropriately for our services. It facilitates communication and relationship building. It also helps encourage consistently compassionate and professional behavior on our part, knowing our words and actions will be seen and interpreted not just by our colleagues, but by laypeople.
As for the anxieties my colleagues often express, again, my own experience of 20 years in an open hospital does not support them. While some clients choose not to watch routine procedures, and most have no interest in seeing their pets have surgery, the vast majority do like to be with their pets during routine exams and when they are hospitalized in our ICU. Cases in which the behavior of the owner interferes with our work are extremely rare, and it is always an option to ask an owner to leave if they do so.
When serious adverse events have occurred with an owner present, from extravasation of chemotherapy drugs to unexpected bleeding during surgery, and even cardiopulmonary arrest, owners have always expressed appreciation for the effort and professionalism of the veterinary team in responding and doing everything possible to help the patient. Without exception, all of the clients I have had over the years who responded to negative outcomes by accusing the team of negligence or incompetence have been clients who were not present to see the care given for themselves.
More studies needed
Of course, anecdotal experience is never a very reliable basis for judging any medical practice. There is very little research evaluating the pros and cons of an open-hospital policy. Studies in human medicine consistently show people want to be with their family members undergoing medical care, and parents in particular see this as an obligation and a right. The limited literature available seems to support the impression that while the idea of this approach engenders some anxiety in healthcare workers, in practice it benefits patients and their family members and does not impede or degrade the care provided.6–8
Even studies of intensive medical procedures, such as family-witnessed CPR, show being present for this type of care has psychological benefits for the family, improves the relationship between family members and the healthcare team, and does not interfere with appropriate treatment of patients.6,9,10 The patient-centered model of care currently widely employed in human medicine recognizes such a policy is an important element of such care and has more benefits than risks. A few studies in veterinary medicine also show that owner-witnessed CPR has positive effects on the owners’ perception of the care given to their pets.11
During the COVID pandemic, our hospital endured the natural experiment of having to suspend our open-hospital policy and keep owners outside of the building while treating their pets. This was universally regarded as more difficult and less satisfactory by both owners and the veterinary team. Communication was more frustrating, patients were often more stressed and less cooperative, and the trust and rapport necessary for an effective functioning VCPR was weakened. While there were some minor benefits to not being constantly observed by clients, these were thoroughly outweighed by the disadvantages of this more distanced arrangement. While the processes necessary during a pandemic do not, of course, fairly represent the normal operations of a hospital without an open-access policy, they did give our team a chance to reflect on the open-hospital experience, and we unhesitatingly and enthusiastically returned to this approach as soon as we safely could.
Bottom line
There is limited evidence objectively evaluating the risks and benefits of allowing pet owners full access to all aspects of their animal companions’ care. Limited relevant research in both human and veterinary medicine suggests caregivers want such access; it is comforting for patients and family members, it supports stronger rapport and communication between the healthcare team and the family, and it does not impede care.
My own personal experience, and that of nearly all the veterinarians and nurses I have worked with in an open-hospital setting, is overwhelmingly positive. There are some potential risks, but these can be mitigated by appropriate policies and good communication. The benefits, to clients, patients, and staff, seem to greatly outweigh these risks. The resistance to this model is based on anxiety and unfamiliarity more than on a realistic understanding of the risks, and I strongly encourage my colleagues to consider a more client-centered care model.
And now, the news
Sadly, I must announce that I am stepping down from both of my EBVM columns here at VPNPlus+ and Veterinary Practice News. It has been my great pleasure to share my passion for evidence-based veterinary medicine and to interact with the outstanding editors and the readers of VPN. I will continue to carry the banner of EBVM into my new work studying aging in dogs, and I look forward to future opportunities to share that work with you.
Brennen McKenzie, MA, MSc, VMD, cVMA, discovered evidence-based veterinary medicine after attending the University of Pennsylvania School of Veterinary Medicine and working as a small animal general practice veterinarian. He has served as president of the Evidence-Based Veterinary Medicine Association and reaches out to the public through his SkeptVet blog, the Science-Based Medicine blog, and more. He is certified in medical acupuncture for veterinarians. Columnists’ opinions do not necessarily reflect those of VPN Plus+.
References
PUN JKH. An integrated review of the role of communication in veterinary clinical practice. BMC Vet Res. 2020;16(1):394. doi:10.1186/s12917-020-02558-2.
Bard AM, Main DCJ, Haase AM, Whay HR, Roe EJ, Reyher KK. The future of veterinary communication: Partnership or persuasion? A qualitative investigation of veterinary communication in the pursuit of client behaviour change. Weary D, ed. PLoS One. 2017;12(3):e0171380. doi:10.1371/journal.pone.0171380.
Yagi K. The Open Practice & Client Presence During Procedures. Clin Br. 2017.
Stellato AC, Dewey CE, Widowski TM, Niel L. Evaluation of associations between owner presence and indicators of fear in dogs during routine veterinary examinations. J Am Vet Med Assoc. 2020;257(10):1031-1040. doi:10.2460/javma.2020.257.10.1031.
Girault C, Priymenko N, Helsly M, Duranton C, Gaunet F. Dog behaviours in veterinary consultations: Part 1. Effect of the owner’s presence or absence. Vet J. 2022;280:105788. doi:10.1016/j.tvjl.2022.105788.
Toronto CE, LaRocco SA. Family perception of and experience with family presence during cardiopulmonary resuscitation: An integrative review. J Clin Nurs. 2019;28(1-2):32-46. doi:10.1111/jocn.14649.
McCabe M. Impact of Family Presence in the Healthcare Setting. 2014. https://core.ac.uk/download/pdf/58825534.pdf. Accessed July 22, 2022.
Beesley SJ, Hopkins RO, Francis L, et al. Let Them In: Family Presence during Intensive Care Unit Procedures. Ann Am Thorac Soc. 2016;13(7):1155-1159. doi:10.1513/AnnalsATS.201511-754OI.
Mark K. Family presence during paediatric resuscitation and invasive procedures: the parental experience: An integrative review: An integrative review. Scand J Caring Sci. 2021;35(1):20-36. doi:10.1111/scs.12829.
Dainty KN, Atkins DL, Breckwoldt J, et al. Family presence during resuscitation in paediatric and neonatal cardiac arrest: A systematic review. Resuscitation. 2021;162:20-34. doi:10.1016/j.resuscitation.2021.01.017.
Gradilla SM, Balakrishnan A, Silverstein DC, Pratt CL, Fletcher DJ, Wolf JM. Owner experiences with and perceptions of owner?witnessed CPR in veterinary medicine. J Vet Emerg Crit Care. 2022;32(3):322-333. doi:10.1111/vec.13180.
Aging in the Dog: Foundations of Canine Geriatric Medicine
What is aging? How we define aging depends on our goals and our frame of reference. From the biomedical perspective of the veterinary clinician, the important elements are:
The passage of time
Deleterious physiologic and functional changes at the molecular, cellular, tissue, and organismal levels
A progressive increase in the risk of the three Ds
Disability
Disease
Death
As dogs age, they lose robustness (the ability to maintain a state of baseline or optimal physiologic function in the face of external stressors) and resilience (the ability to return to this state following perturbations caused by such stressors).1 This leads to frailty and the development of many age-associated diseases which seem superficially unrelated but which are actually all consequences of the same underlying mechanisms of aging.
Is aging a disease? Because aging is a universal phenomenon, at least in mammals, and because historically there have been no effective interventions to slow or stop the aging process per se, only treatments to mitigate the clinical consequences, aging is widely seen as natural, inevitable, and immutable. However, decades of foundational research in laboratory model species, and more limited recent studies in humans and companion dogs, suggest that the core mechanisms of aging can be altered in a way that may prevent the health consequences of aging.2,3 Much debate has focused on the semantic issue of whether or not something natural and ubiquitous but also responsible for illness and death should be labeled a disease.4 There is not yet any consensus resolution to this debate.
A pragmatic approach that avoids this semantic debate is to view aging is the most important modifiable risk factor for disease in companion dogs. This is a familiar concept to veterinarians. Obesity, for example, is a risk factor for multiple specific diseases which increases the overall risk of mortality.5 Focusing on reducing this risk by targeting obesity, rather than waiting for the clinical consequences to develop and then managing each independently is a well-established practice in preventative medicine.
Age-associated changes are responsible for most of the health problems of adult dogs, and there are plausible hypotheses suggesting therapies that could directly target aging and so prevent these problems. The focus of geroscience (the study of the fundamental mechanisms of aging) is to identify these targets and therapies so the field of geriatrics (the clinical management of the aged) can move away from the reactive practice of treating the clinical consequences of aging as they arise and towards a preventative approach of delaying and preventing these consequences by modifying the fundamental processes of aging.
Why do dogs age? It is sometimes supposed that because evolution selects against deleterious traits, the fact that most animals develop disability and disease with age is a paradox. Shouldn’t we have evolved for eternal good health, since this seems obviously more “fit” than getting old and frail?6
One possible explanation for this apparent paradox is that genes and phenotypes which promote reproductive success early in life can cause health problems later in life but still be favored by natural selection.7 Intensive parental investment, for example, may improve reproductive success while simultaneously diminishing the parents reserves and capacity to maintain their own health. Genes favoring such investment would likely outcompete genes favoring parental neglect even if the latter strategy led to longer healthspan and lifespan.
Dogs are also arguably more a product of artificial than natural selection, and many aspects of their aging reflect this. Large and giant-breed dogs, for example, have much shorter lives than smaller breeds, and this is closely tied to genetic differences associated with growth and adult size.8–10
How do dogs age? The cellular and molecular processes associated with aging, and the tissue dysfunction and ultimate health problems that result from these processes, are complex and multifactorial. Research in laboratory species, and in humans and our canine companions, has elucidated many of these mechanisms, and our understanding of them is growing rapidly.1,11–13 Figure 1 illustrated just a few nodes in the complex web of aging.
Figure 1. The web of tissue aging—a partial illustration of the interactions between key tissue-aging mechanisms. GH = Growth hormone. IGF-1 = Insulin-like growth factor-1. From McKenzie (2022)1.
Despite the complexity of aging, it is ultimately just biology, a collection of physiologic processes that can be understood and manipulated like any other. There is a vibrant field of canine geroscience research investigating the processes of aging and potential targets for intervention to extend healthspan and lifespan.
When is a dog “old”? The old canard that every year in a dog’s life is equivalent to seven years for a human is a misleading oversimplification. Dogs age more rapidly than humans at the beginning and end of their life cycles, but the overall lifespan trajectory is quite similar.14 Large and small dogs often age quite differently as well, so the designation of geriatric status may be appropriate much earlier for some breeds than others. In terms of chronological age, or simply the time a dog has been alive, one has to consider size, breed, and individual characteristics. For practical purposes, this approximation is at least useful for triggering more intensive monitoring and investigation of clinical complaints, but it is merely a very rough guide to when we might call a dog “old:”
Small (under 20 lbs) > 12 years
Medium (20-50 lbs) > 10 years
Large (over 50 lbs) > 8 years
More important than chronological age, however, is biological age, defined as the degree to which aging has impacted the robustness, resilience, and state of health and function in an individual as measured by physical, functional, and biomarker assessment.1 We do not yet have reliable tools for measuring biological age, but many are being developed and tested, and ultimately this will be a much more accurate way to predict the age-associated risk of the three Ds (disability, disease, and death) than chronological age.
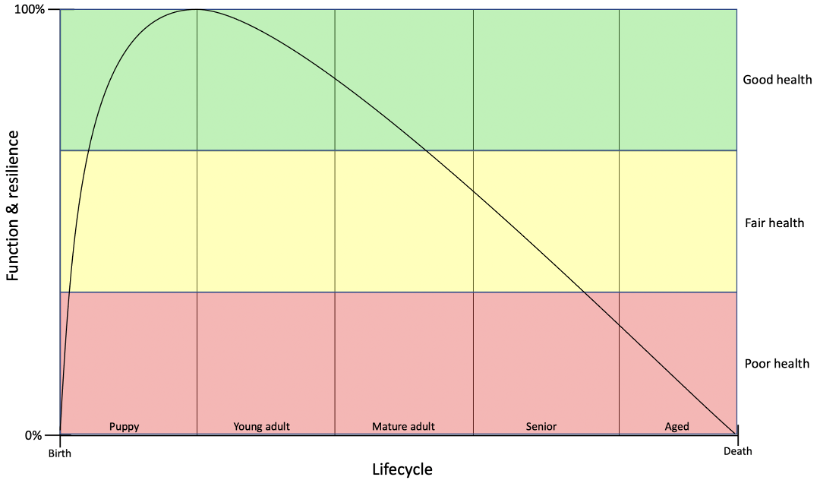
What can we do about canine aging? The ideal response to the burden of aging on the health and wellbeing of dogs and their caregivers is to target the core mechanisms of aging and extend lifespan by preventing the entire array of age-associated diseases and clinical problems. Figure 2 illustrates the goal of extending both lifespan (the time alive) and healthspan (the time without significant age-associated health problems).
a)
b)
Figure 2. Lifespan trajectories in the dog. a) standard trajectory showing gains and declines in robustness and resilience throughout the lifecycle from birth to death. b) trajectory showing the results of therapies targeting core aging mechanisms and resulting in extended lifespan and healthspan and morbidity compressed into a smaller window of time prior to death
Until we have validated therapies to accomplish this, however, we can best serve our canine patients by encouraging lifestyle habits that are known to delay age-associated disease and mortality:
A systematic approach to the geriatric canine patient Once age-associated health problems do develop, we can best care for our patients with systematic, rational, evidence-based assessment and management. There are many tools that allow us to evaluate pain, impaired mobility, frailty, and other manifestations of canine aging, and these are not yet widely and consistently used. Many of the most common age-associated diseases, such as chronic kidney disease, cardiac disease, and many types of neoplasia, have been the focus of extensive research, and there are often clinical practice guidelines and other evidence-based tools to help support high-quality therapeutic management of these conditions.18–20 And finally, despite some significant limitations, the emerging discipline of hospice and palliative care is an important element in caring for those patients most severely affected by aging.21
A systematic approach to geriatric medicine encourages proactive identification of disease and clinical problems and using the bets available evidence to guide diagnostic and treatment interventions. Too often, clinical signs of frailty and disease are dismissed as “just slowing down” or “normal aging” rather than appropriately assessed, monitored, and managed. In the future, proactive and systematic detection of such signs will be a critical element in the determination of biological age and the decision to employ therapies targeting aging directly.
References
1. McKenzie BA, Chen FL, Gruen ME, Olby NJ. Canine Geriatric Syndrome: A Framework for Advancing Research in Veterinary Geroscience. Front Vet Sci. 2022;0:462. doi:10.3389/FVETS.2022.853743
2. Campisi J, Kapahi P, Lithgow GJ, Melov S, Newman JC, Verdin E. From discoveries in ageing research to therapeutics for healthy ageing. Nat 2019 5717764. 2019;571(7764):183-192. doi:10.1038/s41586-019-1365-2
3. Lawler DF, Evans RH, Larson BT, Spitznagel EL, Ellersieck MR, Kealy RD. Influence of lifetime food restriction on causes, time, and predictors of death in dogs. J Am Vet Med Assoc. 2005;226(2):225-231. doi:10.2460/javma.2005.226.225
4. McKenzie BA. Is Aging a Disease? DVM360. 2022;53(3):25.
5. Salt C, Morris PJ, Wilson D, Lund EM, German AJ. Association between life span and body condition in neutered client-owned dogs. J Vet Intern Med. 2019;33(1):89-99. doi:10.1111/JVIM.15367
6. Johnson AA, Shokhirev MN, Shoshitaishvili B. Revamping the evolutionary theories of aging. Ageing Res Rev. 2019;55:100947. doi:10.1016/J.ARR.2019.100947
7. Austad SN, Hoffman JM. Is antagonistic pleiotropy ubiquitous in aging biology? Evol Med Public Heal. 2018;2018(1):287-294. doi:10.1093/EMPH/EOY033
8. Rimbault M, Beale HC, Schoenebeck JJ, et al. Derived variants at six genes explain nearly half of size reduction in dog breeds. Genome Res. 2013;23(12):1985-1995. doi:10.1101/gr.157339.113
9. Plassais J, Rimbault M, Williams FJ, Davis BW, Schoenebeck JJ, Ostrander EA. Analysis of large versus small dogs reveals three genes on the canine X chromosome associated with body weight, muscling and back fat thickness. Clark LA, ed. PLOS Genet. 2017;13(3):e1006661. doi:10.1371/journal.pgen.1006661
10. Kraus C, Pavard S, Promislow DEL. The size-life span trade-off decomposed: Why large dogs die young. Am Nat. 2013;181(4):492-505. doi:10.1086/669665
11. López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. The hallmarks of aging. Cell. 2013;153(6):1194-1217. doi:10.1016/j.cell.2013.05.039
12. Sándor S, Kubinyi E. Genetic Pathways of Aging and Their Relevance in the Dog as a Natural Model of Human Aging. Front Genet. 2019;10:948. doi:10.3389/fgene.2019.00948
13. McKenzie BA. Comparative veterinary geroscience: mechanism of molecular, cellular, and tissue aging in humans, laboratory animal models, and companion dogs and cats. Am J Vet Res. 2022;83(6). doi:10.2460/AJVR.22.02.0027
14. Wang T, Ma J, Hogan AN, et al. Quantitative Translation of Dog-to-Human Aging by Conserved Remodeling of the DNA Methylome. Cell Syst. 2020;11(2):176-185.e6. doi:10.1016/j.cels.2020.06.006
15. Salt C, Morris PJ, Wilson D, Lund EM, German AJ. Association between life span and body condition in neutered client-owned dogs. J Vet Intern Med. 2019;33(1):89-99. doi:10.1111/JVIM.15367
16. McKenzie BA. What does the evidence say about feline fitness and dog aerobics? Vet Pract News. Published online January 2022:25-26.
17. Urfer SR, Wang M, Yang M, Lund EM, Lefebvre SL. Risk Factors Associated with Lifespan in Pet Dogs Evaluated in Primary Care Veterinary Hospitals. J Am Anim Hosp Assoc. 2019;55(3):130-137. doi:10.5326/JAAHA-MS-6763
18. (IRIS) IRIS. Treatment Recommendations for CKD in Dogs.; 2019.
19. Keene BW, Atkins CE, Bonagura JD, et al. ACVIM consensus guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs. J Vet Intern Med. 2019;33(3):1127-1140. doi:10.1111/jvim.15488
20. Biller B, Patel M, Smith D, Bryan C. 2016 AAHA Oncology Guidelines for Dogs and Cats*. J Am Anim Hosp Assoc. 2016;52:181-204. doi:10.5326/JAAHA-MS-6570
21. Bishop G, Cooney K, Cox S, et al. 2016 AAHA/IAAHPC End-of-Life Care Guidelines. J Am Anim Hosp Assoc. 2016;52(6):341-356. doi:10.5326/JAAHA-MS-6637)
As part of my work as Director of Veterinary Medicine for Loyal, a company studying therapies to extend lifespan and delay or prevent age-associated disease in dogs, I am writing regular blog posts. Many of these concern canine aging, though there are some addressing general canine health and biology as well. This is partly responsible for the reduced frequency of my SkeptVet posts, but since many of these may be of interest to followers of this blog as well, I am collecting these posts here just as I did for my VPN column.
As always, feedback is welcome, and if you have subjects you would like to hear more about, let me know!
Should you zoom call your dog? There are now lots of devices that let us call our dogs and say “Hi!” when we aren’t at home. But are these really for our dogs, or just for us? (February, 2022)
Healthspan: the healthy prime of life Lifespan is the amount of time lived. Healthspan is the time lived with vigor and good health. Which do you think is more important? (February, 2022)
Obesity and epigenetics One of the most important health problems in veterinary medicine today is the epidemic of obesity in our pets. (April, 2022)
Signs of senior years: looking old, feeling old, and acting old Do you ever wonder how your dog might look, feel, or act as they advance in age? Understanding aging gives us the potential to prevent or mitigate a wide range of age-related health problems in dogs. (August, 2022)