Over the more than 15 years I have been writing this blog, I have tried to call attention to some individuals who consistently and egregiously disdain science and offer unfounded, potentially dangerous products or advice. This effort, more than any other aspect of the blog, has generated vehement and voluminous hostile response from the individuals themselves and their supporters.
This system is under-resourced and subject to the whims of politics, and it rarely seems to care about whether vets provide treatment that is safe and effective. Most actions taken by veterinary medical boards or the legal system concern administrative or procedural violations, malfeasance involving money or controlled drugs, or other transgressions that are not related to whether the practices an individual sells or advocates actually work. The legal system is notoriously unable to impose any basic standard of care that relies on science, leaving the public at the mercy of the judgement of individuals vets.
While this may seem appropriate (vets should be, after all, better able to judge the legitimacy of medical therapies than judges and lawyers), it provides not even the most basic guardrails against pseudoscience and nonsense. I often find myself wondering what the point is of licensing veterinarians and having a government-sanctioned monopoly on the practice of veterinary medicine if the government is effectively going to let any quack sell nearly any nonsense they like as “medicine.” How does this protect the public?
In this context, it requires some pretty extreme behavior to draw legal or regulatory sanction, and even then such sanction is rarely focused on the unreasonable practice itself but some technical violation of the laws or regulations. And when such sanctions are applied, they seem to rarely hinder the individual from continuing to practice whatever nonsense they favor.
In the past, I have pointed out that, for example, Gloria Dodd was warned and sanctioned for illegal pseudoscientific practices, yet she continued to offer them until her death, and her company continued to do so for some time after that. Jonathan Nyce defrauded people with a fake cancer cure for pets (along with plenty of other sketchy activities) for many years before finally being sentenced to prison. Eric Weisman has been sanctioned by the boards for medicine, veterinary medicine, and chiropractic in his state over decades, yet he is still offering claims and services on his web site that seem inconsistent with the law.
My point in discussing these individuals and their interactions with the legal and regulatory system, then, is clearly not to stop their activities, since I have no power to do so. I simply want the public to understand how extreme these people are. Contrary to the myth they peddle of malign and well-funded Big Pharma or other entrenched interests persecuting these noble folks, who are just trying to help people and their pets, the reality is that it takes a lot for work for a veterinarian to get even a slap on the wrist in the current regulatory environment. These people flout even the minimal standards that exist, and while they undoubtedly believe they are brave to do so, they are really just reckless and a danger to the public.
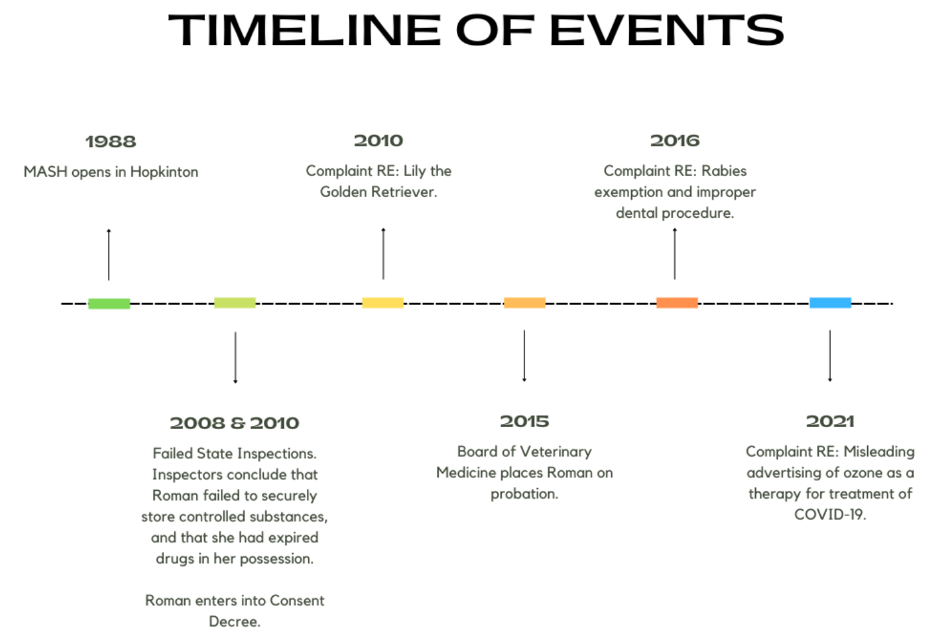
The latest examples include one vet I have written about in the past, Jean Dodds, and another I have been aware of but really not written much about, Margo Roman (apart from a short callout in 2010 when she was selling a nude calendar featuring holistic” veterinarians as a way to raise funds for a series of propaganda videos about alternative veterinary medicine).
Margo Roman Dr. Roman is a proponent of many of the standards of alternative medicine- acupuncture, herbs, homeopathy, etc. She has extreme views on vaccines, diet, and plenty of other subjects. Her particular passions seem to be microbiome-based therapies (derived, of course, from her raw-fed, minimally vaccinated, “chemical-free” dogs) and ozone therapy. It is the latter that most recently got her in trouble with the authorities.
Dr. Roman received a two-year suspension of her veterinary license for recommending to her clients the unscientific and illegal use of ozone to prevent or cure COVID-19. A court decision upheld that sanction. This may seem a drastic action relative to the violation, though it did constitute practicing human medicine without a license, which the government tends to take a bit ore seriously than violations concerning animal patients. However, some investigative reporting has identified a pattern of blatant and egregious behavior that may explain the suspension in this case.
According to this report, has repeatedly been found to have practiced unscientific and ineffective medicine leading to serious patient harm and suffering. A Golden retriever named Lily, who was dying of cancer, was left to suffer after she talked the owners out of euthanasia and employed homeopathy, acupuncture, ozone, and other worthless interventions that clearly had no effect. Another dog was put through a painful dental procedure, with Dr. Roman reportedly filing down many of its teeth and providing no pain control or antibiotics.
She has also been involved in legal action with Tufts University after taking her horse to the veterinary hospital and then refusing to pay for services because the staff was honest about the fact that her alternative therapies were not helping the horse and that the it was suffering. Later she was barred from attending an educational event at the school, which she apparently wanted to attend to challenge the stance of the talk opposing raw diets, since she had refused to pay her bill. The court found her lawsuit in response to be without merit.
Of course, Dr. Roman and her supporters are portraying her as a victim, harassed by entrenched interests that are threatened by her alternative methods. The real victims, however, are the patients she has treated with these methods and their human families, whether they know it or not.
Jean Dodds The other veterinarian recently sanctioned will be much more familiar to readers. Jean Dodds has consistently refused to accept the scientific reality that much of what she advocates is unproven or worthless, such as her Nutriscan allergy testing. She also repeatedly refuses to accept that the government has an authority over what she does as a vet. Despite not having a license to practice veterinary medicine, she offers diagnostic and treatment advice based on the Nutriscan test, and as a result she was cited by the California Veterinary Medical Board for unlicensed practice in 2021. She has continued to do so anyway, and last month she was again cited for unlicensed practice.
The arrogance of not only inventing and selling pseudoscientific tests and treatments but of ignoring the fact that doing so is clearly illegal is really quite stunning. Sadly, when reporting on her 2021 citation I said,
I am not sanguine that there will be any significant consequences for Dr. Dodds stemming from this action…I will not be at all surprised if Dr. Dodds manages to evade responsibility and continue her practices regardless of this action.
Looks like I was right then, and I see little hope that the lates slap on the wrist will change Dr. Dodds’ behavior or shake the confidence of her followers.
A while back I had an enjoyable conversation with Dr. Hubert Hiemstra, who runs the Vet Vault podcast on the Sunshine Coast of Australia. We talked about the changing landscape of veterinary medicine, including economics and science, as well as some of my favorite topics in skepticism, critical thinking, and science-based veterinary medicine. Enjoy!
Aging is the single most important risk factor for disability, disease, and, ultimately, death in adult dogs.1 It has long been viewed as inevitable and immutable, but decades of scientific research have demonstrated aging is more appropriately understood as a modifiable risk factor for these negative health outcomes.
I recently published this article looking at some of the exciting new areas of research in canine aging, including the work I am involved in at Loyal.
A regular feature in my continuing education conference talks for vets is a review of therapies that are popular and they we might want to reconsider based on scientific evidence. Some of these are perennial, such as metronidazole for acute diarrhea or glucosamine for osteoarthritis. Others recommend new fads, such as the burgeoning popularity of gabapentin as a pain reliever.
Below is the proceedings for a version of this talk I gave at the Western Veterinary Conference in Las Vegas earlier this month. A .pdf of the associated slid deck is included at the end.
CHOOSING WISELY: THINGS TO STOP DOING IN YOUR PRACTICE (MAYBE)
THE JOY AND THE PAIN OF EVIDENCE-BASED MEDICINE Veterinary medicine is a science-based profession. The philosophy and principles of science, and the data generated by scientific research, guide our clinical decision-making. The joyful side of this is that we get to watch new tests and treatments emerge during our career, and previously hopeless problems become treatable. The scourge of parvoviral enteritis has been dramatically diminished thanks to the development of a vaccine. The “incurable” malady of feline infectious peritonitis now seems to be beaten, at least in many cases, by new drugs. The first wave of monoclonal antibody therapies is just arriving, offering more treatment options for diverse problems such as osteoarthritis and atopic dermatitis.
The painful side of an evidence-based approach to practice is that we are often wrong. Not only does early and incomplete science sometimes lead us to the wrong conclusions, but as individuals we make even less reliable judgements based on personal experience and anecdote. What is worse, we develop strong emotional and ideological commitments to these judgements. Giving up a therapeutic practice that we believe in, that we were taught as youngsters and that we have since taught to others, that we “have seen work” in our own hands, is deeply unsettling. We don’t like to be wrong, and we don’t like things that challenge our understanding of the world, because that damages our self-image and makes the world seem less predictable and controllable.1,2
But the welfare of our patients is more important than our ego and our sense of security, and we have an obligation as practitioners of a science-based art to follow the evidence where it leads. This will inevitably mean abandoning beliefs and practices that are dear to us repeatedly throughout our careers. So, let’s square our shoulders, raise our chins, and rip off a few of those band aids today!
WHAT IS EVIDENCE? Ok, before we do that, we should take a minute to consider what “evidence” is and how we decide when it is good enough to justify changing our practices.3 You’ve all seen some image like Fig. 1 before. The details are less important than the general point—not all evidence is equally reliable. The bottom of the pyramid contains the most available and accessible evidence– our experiences and opinions and those of others. The top of the pyramid is the smallest because it represents the evidence that’s the hardest to get– consistent findings across multiple, replicated, high-quality controlled research studies. So, we have lots of the least trustworthy evidence and only a little of the best stuff.
Figure 1. Types of evidence categorized by quality and risk of bias.
But the problem is even worse than that! The stuff at the bottom is by far the most psychologically compelling. Our brains are built to understand and trust our own experiences and the stories other people tell us about theirs. Data and numbers from research studies are a lot less satisfying and convincing.4 So we are most confident in the least reliable evidence and least likely to be moved by the evidence that history has shown us, again and again, is most likely to be correct. Bummer!
Science is not, of course, a perfect process. It is simply something humans have developed over a long period of trial and error to compensate for our inherent limitations. Scientific studies can be wrong and misleading, just like anecdotal evidence. Not every study is well-designed, properly conducted and analyzed, and not every study applies to all patient populations. There are a million reasons why scientific research evidence might lead us to the wrong conclusion. But there are ten million reasons why experience and anecdotes will mislead us!
The best we can do is recognize the problem and make an honest effort to remind ourselves often that what feels true may not be if it is based on uncontrolled experience and anecdote. If you find yourself saying, “But, I’ve seen it work!” take a deep breath and try to remind yourself that the proponents of blood-letting, magic healing rituals, and any therapy you believe is useless say exactly the same thing.
USES OF ANTIBIOTICS TO RECONSIDER Treatment of Acute Diarrhea The use of metronidazole as a treatment for acute diarrhea in dogs is a deeply entrenched practice that goes back decades. Various rationales have been proposed to support it, from treatment of potential bacterial causes, such as Clostridium, to anti-inflammatory mechanisms. Few general practice vets have not used this drug for this purpose, and there is abundant anecdotal evidence suggesting it is beneficial.
Unfortunately, there is also a growing body of research evidence showing little to no clinical benefit for most patients and some potential undesirable effects.5 At best, it might shorten the course of diarrhea by about a day. At worst, it can make symptoms worse, disrupt the microbiome in potentially harmful ways, and contribute to antibiotic resistance.
Given that the vast majority of dogs with idiopathic acute diarrhea will get better with time, these risks are hard to justify. Most humans don’t seek medical are or prescription drugs for mild, short-term diarrhea symptoms. The pressure to treat this condition in dogs has more to do with the inconvenience and anxiety it causes owners than the wellbeing of our patients. Although the risks seem small, it is difficult to justify them for a treatment that has mostly psychological benefits for vets and clients rather than medical benefits for patients.
It would be nice to have a clear alternative to offer here, but the reality is no research yet supports any specific treatment for acute, self-limiting diarrhea that is clearly effective and has negligible risks. Probiotics have not entirely lived up to their promise.6 Some evidence supports dietary change and fiber supplementation,7,8 but again most cases are self-limiting and likely to get better without any specific treatment.
Treatment of Upper Respiratory Infections Like acute diarrhea, acute upper respiratory infections (URI) are often self-limiting in dogs and cats, and many have viral etiologies which will not respond to antibiotic treatment. There is limited controlled research comparing antibiotic use to alternatives, such as supportive care alone. Based on the clinical research that we do have, and also the basic science studies providing background on the causes and outcomes of feline and canine upper respiratory disease, expert consensus guidelines generally recommend limiting antibiotic use to cases with significant systemic symptoms (e.g. fever, lethargy) and evidence of bacterial involvement (e.g. mucopurulent discharge), or cases with chronic disease.9
Unfortunately, the lack of evidence for benefits from antibiotic treatment in most cases, and the potential for adverse effects and microbial resistance, vets still seem to often prescribe antibiotics unnecessarily for canine and feline respiratory infections.10,11 There is some indication, however, that awareness of, and adherence to, antibiotic use guidelines may be improving.12
Treatment of Urinary Tract Infections Unlike upper respiratory disease, urinary tract symptoms often are caused by bacterial infection in dogs, and to a lesser extent in cats. These bacterial urinary tract infections (UTI) do sometimes require antibiotic treatment, though common practice in treating UTIs still often does not match current evidence-based guidelines.13
For one thing, just having bacteria in the urine does not a UTI make. Asymptomatic bacteriuria seems to be more common than previously recognized, occurring in from 1% to 13% of healthy dogs and cats, and at much higher rates in animals with immunosuppressive conditions or medications and other risk factors.13 In the absence of clinical symptoms, treatment with antibiotics does not permanently eliminate bacteriuria and appears to have no benefits for the patient. While evidence is somewhat limited in dogs and cats, it is clear that in humans prescribing antibiotics for subclinical bacteriuria raises the risk of adverse drug effects and antibiotic resistance without improving short-term or long-term outcomes for patients. This is true even if there is pyuria!13
Recommended treatment of symptomatic UTI confirmed by urine culture is also different from what many of us were taught long ago. Some of these cases may not require antibiotics at all. Humans with uncomplicated UTI are often treated symptomatically with NSAIDs, and the UTI often resolves by itself. This may be appropriate for veterinary patients too, though we do not yet have studies showing this.
Similarly, the recommended duration of treatment is 3-5 days, which is far shorter than the 7-10 day course many of us still prescribe. Even pyelonephritis is typically treated in humans with 7-10 days of antibiotics, and in the absence of better evidence experts currently recommend 10-14 days of treatment in dogs and cats, rather than the 4-6 weeks previously advised.13
One of the most common inappropriate uses of antibiotics for urinary tract signs is for young cats. In cats under about ten years of age hematuria, pollakiuria, and other symptoms of cystitis are far less likely to be caused by UTI (2%-19%) than in cats over 10 years of age (40-45%).14 Feline Interstitial Cystitis (FIC) is the most common cause of lower urinary tract symptoms, and of course antibiotics are not a useful or appropriate treatment for cats with FIC.15
Much of the antibiotic prescribing for urinary tract symptoms, as for gastrointestinal and respiratory symptoms, is driven by psychological factors: owner anxiety and demands for treatment, veterinarian anxiety about negative consequences to undertreating, and simple commission bias (the need to DO SOMETHING rather than wait for self-limiting problems to resolve on their own).4 Given that antibiotics are safe but not entirely benign, and that we are losing some effective treatments for serious infections to antimicrobial resistance, we should do what we can to resist the siren-song of antibiotic prescription above and beyond what is likely needed.
Perioperative Antibiotics Speaking of anxiety, the prospect of a post-operative infection appears to haunt the nightmares of veterinarians, based on the rate at which many of us prescribe antibiotics for our surgical patients.
Available evidence suggests that surgical site infections are uncommon for most clean or clean-contaminated procedures (< 5%), and that giving antibiotics before or after surgery do nothing to prevent these. Even in cases with specific risk factors for infection, the most we should likely do is provide appropriate antibiotic coverage from 30-60 minutes before the procedure until 6 to 24 hours afterwards.16 There is no convincing rationale or evidence, from human or veterinary medicine, to support more extensive antibiotic use to prevent surgical site infections.
Veterinary dentistry is a special case of perioperative antibiotic use.17 Once again, extensive evidence in human medicine shows that bacteremia occurs with chewing, brushing, or flossing just as it does with dental procedures, and that antibiotics are not useful for routine prophylactic procedures. Only people at high risk of infective complications (those with implant foreign bodies, a history of certain cardiac diseases, or those who are immunosuppressed) are likely to benefit from antibiotics when having dental work.
There is a lot less data in veterinary patients, but the expert consensus is that antibiotics are rarely necessary for dentistry patients and are not justified except in those at high risk. Unfortunately, it isn’t clear who those patients are. Infective endocarditis is often suggested as a potential risk from dental procedures, but this appears to be extremely rare in dogs and cats. Overall, antibiotics are very unlikely to benefit the vast majority of veterinary dentistry patients, and their risks likely outweigh their benefits.17
Despite this, it appears that antibiotics are very commonly used in veterinary dentistry. In dogs and cats with established periodontal disease or requiring extractions (which describes most dentistry patients), antibiotic use appears to be very common, though use
varies widely between different veterinary facilities.18 More evidence and clearer guidelines would likely help reduce the overuse of antibiotics in veterinary dentistry.
USES OF ANALGESICS TO RECONSIDER Gabapentin The authors of the 2022 American Animal Hospital Association pain management guidelines for dogs and cats, at least, are trying to prevent history from repeating itself. They state, “Gabapentin has become the new tramadol, with widespread usage [despite] virtually no supporting data.”19
While there is good evidence in humans to support use of gabapentin for seizures and for some specific types of neuropathic pain (post-herpetic neuralgia and diabetic neuropathy), even most analgesic use in humans is without much supporting research evidence.20 In dogs and cats, there is limited evidence to support using gabapentin to reduce behavioral signs of stress, although it isn’t entirely clear if it reduces anxiety or is primarily a sedative. However, there is little reason to expect it to be of great benefit for acute or chronic pain. While more research needs to be done, it seems likely we have failed to learn our lesson from tramadol and are continuing down a similar road with this drug.
Local Anesthetics Mixing Lidocaine and Bupivicaine for Local Blocks This is one of those ideas that sounds brilliant but is actually totally wrong!21 Some clinicians mix lidocaine and bupivacaine together with the idea that they will get “the best of both worlds–” the more rapid onset of lidocaine with the longer duration of bupivacaine. What actually happens is that you get the worst of both worlds!
The dilution of each drug leads to a lower concentration gradient, meaning less of both end up getting into the nerves where they act to block pain. The difference in pH also means that mixing them likely slows the uptake of the lidocaine and might make the bupivacaine more likely to precipitate. Clinical studies in actual human and veterinary patients have also shown that this practice does not reduce the time to effect, but it does shorten the duration.
Nocita (liposomal encapsulated bupivacaine) This is a product that has been FDA approved for use in dogs undergoing stifle surgery and cats being declawed, but it is widely used for many other surgical situations. Last year, three studies were published comparing this product to a saline placebo in dogs undergoing a laparotomy or other soft-tissue surgery.22–24None found liposomal bupivacaine to be superior to placebo! Now, there are a variety of possible explanations besides the obvious–that it doesn’t work for these types of surgeries—but that is at least a possible explanation to be considered. There are studies showing this product is as effective as regular bupivacaine, so arguably it may be more cost effective to use a non-liposomal product until it becomes clear why these studies were negative. However, that raises the question if Nocita was as good as regular bupivacaine but no better than placebo, does regular bupivacaine, or the other common local anesthetics, even work?!
Local Anesthetics for routine soft-tissue surgery A large number of studies have been done comparing various local anesthetics to each other or placebo, and these have involved a tremendous variety of local techniques, surgical procedures, assessment measures, and other analgesics. A comprehensive survey of this literature would be a massive project fit for a PhD thesis, but a survey of just those studies published since 2018 and just involving laparotomy or other soft-tissue procedures provide a representative sample of this vast literature.22,25–35
Some of these studies show a beneficial effect of local anesthetics and many do not. Overall, the literature is weak and inconsistent, which is surprising given the widespread presumption that these drugs are meaningfully effective. The clinical takeaway from this inconsistency is that local anesthetics may add some small analgesic benefit, but they are not to be relied on as the sole analgesic or as a substitute for systemic analgesia.
Steroids for Intervertebral Disk Disease (IVDD) Acute medical management of IVDD mostly involves controlling pain and trying to prevent further injury or loss of function. Steroids have long been used for both analgesia and to protect from further deterioration of nerve tissue by reducing inflammation. Unfortunately, it has been difficult to produce research evidence that supports the real-world benefits of this approach. In humans, the use of oral steroids does not appear very beneficial, though it does have a higher incidence of adverse effects than other analgesics. The evidence in veterinary patient is sparse, but the most recent ACVIM consensus statement on the subject indicates that:36
there is limited evidence that corticosteroid use is associated with poorer outcome and decreased quality of lifeas well as a higher rate of recurrence compared to nonsteroidal anti-inflammatory drugs (NSAIDs)
[there is] insufficient evidence to support corticosteroid use for neuroprotective purposes
In a retrospective study, dogs receiving NSAIDs had higher quality of life scores than those receiving corticosteroids
there is not sufficient evidence to support the use of corticosteroids as a protective strategy against the development of progressive myelomalacia
The best we can say is that steroids are probably no better than NSAIDs, and it seems likely they may be worse.
MISCELLANEOUS TREATMENTS TO RECONSIDER ACE Inhibitors for Pre-clinical Mitral Valve Disease Diagnosis and staging of mitral valve disease (MMVD) before dogs are in congestive heart failure (CHF) is now pretty rewarding. The advent of pimobendane has given us an intervention that likely delays the onset of CHF and extend life significantly for dogs with this disease.37 It wasn’t always so.
Back in the Dark Ages that make up most of my career, we used to give these dogs ace inhibitors (ACE-I). There were some sound theoretical arguments to suggest this would slow the progression to CHF. Unfortunately, a few pesky scientists weren’t satisfied with theory, and they did some clinical studies in actual MMVD patients. They found that that we were most likely wasting our time.
As the most recent systematic review puts it, “Administration of angiotensin-converting enzyme inhibitors to dogs with preclinical myxomatous mitral valve disease…results in little to no difference in the risk of the development of congestive heart failure and may result in little to no difference in cardiovascular-related and all-cause mortality.”38
Good thing we’ve all stopped doing this, eh?
Glucosamine for Osteoarthritis (OA) Probably the most popular (and profitable!) supplement in the history of veterinary medicine is glucosamine, alone or mixed with chondroitin or other agents. If everyone has used it forever, it has to work, right?!
Well, it turns out there is some controversy about that. Decades of research, hundreds of studies, are currently summarized in dozens of systematic reviews over the last ten years. For humans, these are often broken down into treatment for OA in specific joints, and there is sometimes analysis of glucosamine alone, in combination with other agents, or in different formulations and dosages. The result is muddled, and no clear, universal conclusions are possible.
About 60% of the reviews conclude there is some benefit to some type of glucosamine-containing product, and the other 40% conclude no meaningful benefit or insufficient evidence to tell. Not exactly a ringing endorsement for one of the most widely used supplements ever. The most recent systematic review for veterinary patients is ambivalent:39
“As we exposed in this review, glucosamine and chondroitin sulfate seems to provide chondroprotective effects and less inflammatory biochemical response in approximately half of the evaluations. However, these effects are inconsistent between the clinical and the preclinical studies… a possible caregiver placebo effect may explain some of the beneficial responses observed in clinical trials with dogs.”
The latest guideline from the American College of Rheumatology and the Arthritis Foundation, “recommends against glucosamine alone or with chondroitin because treatment does not improve knee and hip OA in studies without industry funding.”40 Ouch!
The American Academy of Orthopedic Surgeons say glucosamine “May be helpful in reducing pain and improving function…however, the research is inconsistent/limited.”41
There aren’t official guidelines from specialty groups in veterinary osteoarthritis management, but a recent proposed expert consensus statement highlighted the “lack of evidence” for efficacy needed to draw a firm conclusion.42 Another similar consensus statement indicated that three or four of nine contributing experts recommended offering some form of glucosamine for patients with OA depending on the specific circumstances.43
Despite being widely used for decades, it has proven impossible to clearly demonstrate that glucosamine in some form or combination has meaningful benefits for comfort and function in veterinary patients with OA. It is pretty well demonstrated to be safe, so there is unlikely to be any direct harm from using it. However, if it is ultimately not truly beneficial, what a horrendous waste of money it will have been for owners. And if it is used in place of clearly beneficial treatments (as it likely is, given how phobic people often are about NSAIDs), many OA patients could be suffering unnecessarily.
References
1. Burton RA. On Being Certain: Believing You Are Right Even When You’re Not. 1st ed. St. Martin’s Press; 2008. Accessed April 3, 2024. http://catdir.loc.gov/catdir/enhancements/fy0829/2008001470-s.html
2. Gilovich T. How We Know What Isn’t so: The Fallibility of Human Reason in Everyday Life. 1. Free Press paperback ed. Free Press; 1993.
3. McKenzie B. Evidence-based veterinary medicine: What is it and why does it matter? Equine Vet Educ. 2014;26(9):451-452. doi:10.1111/eve.12216
4. McKenzie BA. Veterinary clinical decision-making: cognitive biases, external constraints, and strategies for improvement. J Am Vet Med Assoc. 2014;244(3):271-276. doi:10.2460/javma.244.3.271
5. Scahill K, Jessen LR, Prior C, et al. Efficacy of antimicrobial and nutraceutical treatment for canine acute diarrhoea: A systematic review and meta-analysis for European Network for Optimization of Antimicrobial Therapy (ENOVAT) guidelines. Vet J. 2024;303:106054. doi:10.1016/j.tvjl.2023.106054
6. Jensen AP, Bjørnvad CR. Clinical effect of probiotics in prevention or treatment of gastrointestinal disease in dogs: A systematic review. J Vet Intern Med. 2019;33(5):1849-1864. doi:10.1111/jvim.15554
7. Lappin MR, Zug A, Hovenga C, Gagne J, Cross E. Efficacy of feeding a diet containing a high concentration of mixed fiber sources for management of acute large bowel diarrhea in dogs in shelters. J Vet Intern Med. 2022;36(2):488-492. doi:10.1111/jvim.16360
8. Moreno AA, Parker VJ, Winston JA, Rudinsky AJ. Dietary fiber aids in the management of canine and feline gastrointestinal disease. J Am Vet Med Assoc. 2022;260(S3):S33-S45. doi:10.2460/javma.22.08.0351
9. Lappin MR, Blondeau J, Boothe D, et al. Antimicrobial use Guidelines for Treatment of Respiratory Tract Disease in Dogs and Cats: Antimicrobial Guidelines Working Group of the International Society for Companion Animal Infectious Diseases. J Vet Intern Med. 2017;31(2):279-294. doi:10.1111/jvim.14627
10. Bollig ER, Granick JL, Webb TL, Ward C, Beaudoin AL. A quarterly survey of antibiotic prescribing in small animal and equine practices—Minnesota and North Dakota, 2020. Zoonoses Public Health. 2022;69(7):864-874. doi:10.1111/zph.12979
11. Robbins SN, Goggs R, Lhermie G, Lalonde-Paul DF, Menard J. Antimicrobial Prescribing Practices in Small Animal Emergency and Critical Care. Front Vet Sci. 2020;7. doi:10.3389/fvets.2020.00110
12. Farrell S, Bagcigil AF, Chaintoutis SC, et al. A multinational survey of companion animal veterinary clinicians: How can antimicrobial stewardship guidelines be optimised for the target stakeholder? Vet J. 2024;303:106045. doi:10.1016/j.tvjl.2023.106045
13. Weese JS, Blondeau J, Boothe D, et al. International Society for Companion Animal Infectious Diseases (ISCAID) guidelines for the diagnosis and management of bacterial urinary tract infections in dogs and cats. Vet J. 2019;247:8-25. doi:10.1016/j.tvjl.2019.02.008
14. Dorsch R, Teichmann-Knorrn S, Sjetne Lund H. Urinary tract infection and subclinical bacteriuria in cats: A clinical update. J Feline Med Surg. 2019;21(11):1023-1038. doi:10.1177/1098612X19880435
15. He C, Fan K, Hao Z, Tang N, Li G, Wang S. Prevalence, Risk Factors, Pathophysiology, Potential Biomarkers and Management of Feline Idiopathic Cystitis: An Update Review. Front Vet Sci. 2022;9:900847. doi:10.3389/fvets.2022.900847
16. Williams J. Antimicrobial prophylaxis: The why and how of antimicrobial prophylaxis. BSAVA Companion. 2018;2018(11):4-7. doi:10.22233/20412495.1118.4
17. Davis E. The Use of Antibiotics in Veterinary Dentistry. Today’s Veterinary Practice. April 14, 2023. Accessed April 3, 2024. https://todaysveterinarypractice.com/dentistry/antibiotics-in-veterinary-dentistry/
18. Weese JS, Battersby I, Morrison J, Spofford N, Soltero-Rivera M. Antimicrobial use practices in canine and feline dental procedures performed in primary care veterinary practices in the United States. PLOS ONE. 2023;18(12):e0295070. doi:10.1371/journal.pone.0295070
19. Gruen ME, Lascelles BDX, Colleran E, et al. 2022 AAHA Pain Management Guidelines for Dogs and Cats. J Am Anim Hosp Assoc. 2022;58(2):55-76. doi:10.5326/JAAHA-MS-7292
20. Chincholkar M. Gabapentinoids: pharmacokinetics, pharmacodynamics and considerations for clinical practice. Br J Pain. 2020;14(2):104-114. doi:10.1177/2049463720912496
21. Hoffmeister E. Mixing local anesthetics – yay or nay? North American Veterinary Anesthesia Society. September 27, 2019. Accessed April 3, 2024. https://www.mynavas.org/post/mixing-local-anesthetics-yay-or-nay
22. Hollenbeck DL, Knue JD, Simon BT, Jeffery ND, Thieman Mankin KM, Dickerson VM. Use of peri-incisional liposomal bupivacaine was not different than placebo regarding pain score or rescue analgesia in a randomized clinical trial of 83 dogs. J Am Vet Med Assoc. Published online January 22, 2025:1-7. doi:10.2460/javma.24.09.0589
23. Hixon LP, Wallace ML, Appleton-Walth K, et al. Bupivacaine liposomal injectable suspension does not provide improved pain control in dogs undergoing abdominal surgery. J Am Vet Med Assoc. 2024;262(2):1-9. doi:10.2460/javma.23.05.0271
24. Middlestead DK, Roa DM, Burgess RCF. A randomized, blinded, placebo-controlled, prospective clinical study to evaluate the effectiveness of a diluted liposomal-encapsulated bupivacaine suspension in dogs undergoing a ventral midline celiotomy. Can Vet J Rev Veterinaire Can. 2024;65(1):59-65.
25. Vicente D, Bergström A. Evaluation of intraoperative analgesia provided by incisional lidocaine and bupivacaine in cats undergoing ovariohysterectomy. J Feline Med Surg. 2018;20(10):922-927. doi:10.1177/1098612X17735167
26. Fudge JM, Page B, Mackrell A, Lee I. Evaluation of targeted bupivacaine for reducing acute postoperative pain in cats undergoing routine ovariohysterectomy. J Feline Med Surg. 2020;22(2):91-99. doi:10.1177/1098612X19826700
27. Nejamkin P, Landivar F, Clausse M, et al. Evaluation of analgesic, sympathetic and motor effects of 1% and 2% lidocaine administered epidurally in dogs undergoing ovariohysterectomy. Vet Anaesth Analg. 2020;47(6):797-802. doi:10.1016/j.vaa.2020.07.034
28. Josso M, Topie O, Bencharif D, Doran DH, Desbois C, Touzot-Jourde G. Ultrasound-Guided Rectus Abdominis Sheath Block in Cats Undergoing Ovariectomy: A Prospective, Randomized, Investigator-Blinded, Placebo-Controlled Clinical Trial. Open Access J Vet Sci Res. 7(1). doi:DOI: 10.23880/oajvsr-16000218
29. Viscasillas J, Cañón A, Hernández E, et al. Clinical Assessment of Introducing Locoregional Anaesthesia Techniques as Part as the Intraoperative Analgesia Management for Canine Ovariohysterectomy in a Veterinary Teaching Hospital. Anim Open Access J MDPI. 2022;12(15):1939. doi:10.3390/ani12151939
30. Garbin M, Ruel HL, Watanabe R, Malo A, Monteiro BP, Steagall PV. Analgesic efficacy of an ultrasound-guided transversus abdominis plane block with bupivacaine in cats: a randomised, prospective, masked, placebo-controlled clinical trial. J Feline Med Surg. 2023;25(2):1098612X231154463. doi:10.1177/1098612X231154463
31. Heitzmann V, Bettschart-Wolfensberger R, Torgerson P, Goldinger E, Palumbo C, Steblaj B. How painful are cats after neutering – a field study using multimodal analgesia with intraperitoneal ropivacaine in a neuter-return program in feral cats. Swiss Arch Vet Sci. 164(4):841-850. doi:https://doi.org/ 10.17236/sat00377
32. Brioschi FA, Ravasio G, Ferrari F, et al. Comparison of intraperitoneal and incisional lidocaine or ropivacaine irrigation for postoperative analgesia in dogs undergoing major abdominal surgeries. PloS One. 2023;18(4):e0284379. doi:10.1371/journal.pone.0284379
33. Kazmir-Lysak K, Steblaj B, Torgerson PR, Kutter APN, Restitutti F, Henze IS. Intraperitoneal and incisional ropivacaine did not improve postoperative analgesia after multimodal anaesthesia compared with saline in dogs undergoing ovariohysterectomy. Schweiz Arch Tierheilkd. 2023;165(10):634-643. doi:10.17236/sat00405
34. Gomes VH, Peixoto AJ, EdosSL Fernandes M, de Souza Campos AC, Coelho CM, da Silva MF. Evaluation of lidocaine administration into the ovarian pedicle for the control of intraoperative and early postoperative pain during ovariohysterectomy in dogs. Vet Anaesth Analg. 2024;51(1):64-70. doi:10.1016/j.vaa.2023.07.002
35. Lawler BM, Guedes AGP, Tearney CC, et al. Evaluation of preoperative intraperitoneal injection of bupivacaine for intraoperative antinociception in cats undergoing ovariohysterectomy: A randomized clinical trial. Res Vet Sci. 2024;180:105439. doi:10.1016/j.rvsc.2024.105439
36. Olby NJ, Moore SA, Brisson B, et al. ACVIM consensus statement on diagnosis and management of acute canine thoracolumbar intervertebral disc extrusion. J Vet Intern Med. 2022;36(5):1570-1596. doi:10.1111/jvim.16480
37. Boswood A, Häggström J, Gordon SG, et al. Effect of Pimobendan in Dogs with Preclinical Myxomatous Mitral Valve Disease and Cardiomegaly: The EPIC Study-A Randomized Clinical Trial. J Vet Intern Med. 2016;30(6):1765-1779. doi:10.1111/jvim.14586
38. Angiotensin?converting enzyme inhibitors in preclinical myxomatous mitral valve disease in dogs: systematic review and meta?analysis – Donati – 2022 – Journal of Small Animal Practice – Wiley Online Library. Accessed April 3, 2024. https://onlinelibrary.wiley.com/doi/10.1111/jsap.13461
39. Barbeau-Grégoire M, Otis C, Cournoyer A, Moreau M, Lussier B, Troncy E. A 2022 Systematic Review and Meta-Analysis of Enriched Therapeutic Diets and Nutraceuticals in Canine and Feline Osteoarthritis. Int J Mol Sci. 2022;23(18):10384. doi:10.3390/ijms231810384
40. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020;72(2):149-162. doi:10.1002/acr.24131
41. Brophy RH, Fillingham YA. AAOS Clinical Practice Guideline Summary: Management of Osteoarthritis of the Knee (Nonarthroplasty), Third Edition. JAAOS – J Am Acad Orthop Surg. 2022;30(9):e721. doi:10.5435/JAAOS-D-21-01233
42. Mosley C, Edwards T, Romano L, et al. Proposed Canadian Consensus Guidelines on Osteoarthritis Treatment Based on OA-COAST Stages 1–4. Front Vet Sci. 2022;9. doi:10.3389/fvets.2022.830098
43. Cachon T, Frykman O, Innes JF, et al. COAST Development Group’s international consensus guidelines for the treatment of canine osteoarthritis. Front Vet Sci. 2023;10:1137888. doi:10.3389/fvets.2023.1137888
I have written a few times in the past about one of the most powerful, and richest, promoters of pseudoscience in the world, Joseph Mercola. More often, I have written about his veterinarian accomplice, Dr. Karen Becker. For many years, Dr. Becker promoted a wide range of unscientific ideas and products in collaboration with Mercola’s online empire. Recently, they have apparently parted ways, though it sounds as if this was not Dr. Becker’s choice.
After 15 years of seamless collaboration and communication…the new executive leadership insisted I sign a non-disclosure agreement…When I hesitated and questioned this…they stopped paying me…
Due to professional, ethical, moral, and spiritual differences, I have no choice but to no longer associate with Mercola.com…I will always be grateful for the opportunity I had through Dr. Mercola and his former executive staff to forward my mission…
In her statement, Dr. Becker referenced some information uncovered by journalists about both changes in the management of Mercola’s empire and also the role a self-professed “channeler” has in advising him. Apparently, Mercola has gotten too crazy (or at least too publicly crazy) for Dr. Becker, though presumably she didn’t know this when she was still collaborating him and before he stopped paying her and shut down her YouTube channel.
Jonathan Jarry at the McGill University Office for Science and Society has done the painful but important work of wading through numerous video recordings of Mercola and his supernatural advisor, and he has provided some terrifying revelations. I have included the full video at the end of this post, but here is one especially disturbing moment:
Current events, especially in the U.S., are stark reminders that proponents of alternative medicine and opponents of science-based medicine are not always merely misguided or harmless. They can be quite bizarre and frankly dangerous. This danger only rarely comes from the kind of violence Mercola proposes. More often, it comes from discouraging the use of truly safe and effective medical care, from vaccines to antibiotics, and from the use of frequently ineffective, and sometimes outright harmful alternatives.
Dr. Becker is clearly not deranged. As I have said many, many times, she is undoubtedly a smart and caring person committed to her beliefs about what is best for companion animals. She is also, however, just as genuinely committed to mistaken beliefs about science and medicine which can cause harm. And she has participated, much more indirectly and cautiously than Mercola, in the demonization of science-based medicine and veterinarians who promote it, while decrying the criticism she receives.
She characterizes cancer therapy in this way-
So, we’re waiting until these animals get cancer and then we have to talk about cutting it out, poisoning it out with chemotherapy, or burning it out with radiation.
Referring to, among other things, pet food, parasite prevention, and vaccines, she has said,
the two big sources of toxins for pets in North America come from the immediate home environment and the veterinarian.
and also
Vaccinosis is a problem only holistic veterinarians seem willing to acknowledge…Since the introduction of dog and cat vaccines, the traditional view of their use has been that they are safe and can be given as frequently as once or twice a year. This approach, tragically, has caused a tremendous amount of suffering for millions of pets.
She feeds the myth of vets as part of a malign industry that profits off of illness and so is not truly motivated to keep pets well:
many traditionally trained DVMs practice ‘reactive’ veterinary medicine. This means they don’t have much to offer pets unless and until they’re good and sick…
And she holds mystical, unscientific views such as this:
Animals innately know what they need to heal themselves. Wild animals have access to Nature’s pharmacy, but our pets don’t. As doctors we dictate what medicine our patients will receive and at what dose. But we often prescribe incorrectly, with disastrous results.
While being certainly much more sane and reasonable than Mercola, Dr. Becker has been his ally for many years, and they have shared a world view that portrays most veterinarians as misguided, misinformed, and even outright dangerous to the health of pets. I am glad she hasn’t taken the next step into madness Mercola has, calling for the “destruction” of the veterinary profession, and that she has parted company with his organization. However, she is not entirely without responsibility for feeding less blatant but still harmful myths along the road to this destination.
Pseudoscience and attacks on science, however nicely packaged, damage the health of our pets and make work and life much harder for the majority of vets committed to scientific medicine. While Dr. Becker and her colleagues will undoubtedly continue to suggest that my criticism of their work is unkind and hurtful, this is disingenuous when so much of what they do is based on attacking science-based veterinary medicine and undermining public confidence in veterinarians.
A fundamental principle of science and skepticism is that substantive criticism of ideas is the only path to weeding out the false and ineffective and bringing humanity closer to a truer, and more useful understanding of nature. We should always be kind and respectful to persons, but attacking their bad ideas is not the same as attacking them personally. As Tom Nichols has put it,
Americans no longer distinguish the phrase “you’re wrong” from the phrase “you’re stupid.” To disagree is to disrespect. To correct another is to insult. And to refuse to acknowledge all views as worthy of consideration, no matter how fantastic or inane they are, is to be closed-minded.
Shifting the focus from ideas to persons is not simply counterproductive, it can lead to the kind of dark places Dr. Mercola has clearly reached, where passionate disagreement about what is true becomes hatred and intolerance of those with whom we disagree.
However, this cannot lead to acceptance or tolerance of harmful beliefs and ideas or we will be forever trapped in a world of conflicting opinions with no solid basis for productive action. Science has drastically improved the lives and health of humans and our animal companions, and the current ascendancy of those who deny this, even when they are not manifestly insane as individuals, hams us and our pets.
Now, more than ever, it is necessary to advocate vigorously for science and the scientific approach to health. We should do so constructively and civility, but we cannot surrender to the rising tide of health practices based on anecdote and opinion, conspiracy and personal faith, mysticism and pseudoscience.
I recently participated in a free webinar discussing neutering of dogs and cats (always a hot-button topic!). I made a screen recording of my segment of the presentation, which I am posting here.
There were some technical glitches, including some popup notifications that I have only been able to hide imperfectly. I was also asked at the last minute to shorten the presentation by 10 minutes, so it’s a bit rushed and doesn’t flow perfectly, and it ends abruptly since I handed over quite quickly to the next speaker. Nevertheless, I hope there will be some useful concepts and information in there for you!
With the dozens of posts covering hundreds of scientific publications and my own experience with acupuncture trainingand practice, I have surely exhausted the subject. Right? Well, in my own mind I have since it is clear to me that acupuncture is founded on a combination of folk mythology and unreliable science, and it almost certainly does little to nothing useful for our pets.
That said, it is still accepted as beneficial by plenty of vets and pet owners, largely on the basis of unreliable anecdotal evidence and an enormous, though ultimately unconvincing, scientific literature. Therefore, I feel obliged to continue my occasional, and almost certainly futile, efforts to protect pets and their owners from wasting time and money, and failing to effectively treat serious medical problems, by employing acupuncture.
A recent study of acupuncture as a treatment for pain in dogs after ovariohysterectomy (spay surgery) reinforces the case against this practice-
The investigators compared pain scores in dogs after spay surgery between two groups of dogs: all getting the standard treatment (an opioid called butorphanol, a sedative called medetomidine, general anesthesia, and an NSAID called meloxicam), some randomly assigned to “electroacupuncture” (electrical stimulation through needs at purported acupuncture points, though these don’t really exist) and “fake” electroacupuncture (needles at the same locations not actually penetrating the skin). The pain assessment was don’t by vets who were, in theory, unable to tell which group got the real and which the fake acupuncture (the needles were passed through a piece of opaque foam so the skin underneath couldn’t be seen).
The result was no difference in pain scores between the groups at any point. Some dogs did show evidence of increased discomfort shortly after surgery, and this was likely due to the use of butorphanol, which is a weak and short-acting opioid and no longer considered adequate for use in a surgical procedure like this.
Of course, negative findings like this never convince believers in acupuncture, and the results didn’t disturb the investigators at all. They simply pointed out positive findings in other studies and came up with a list of excuses- the wrong length of time for treatment, treatment during general anesthesia, possible interference from drugs used, etc. Every possible explanation except for the most plausible- acupuncture is nonsense and doesn’t reduce pain except through placebo effects!
Do you trust your vet? How much? It turns out your answer may well be a good predictor of how likely your dog or cat is to be appropriately vaccinated.
“a large minority of dog owners consider vaccines administered to dogs to be unsafe (37%), ineffective (22%), and/or unnecessary (30%).
A slight majority of dog owners (53%) endorse at least one of these three positions.”
48% of dog owners opposed mandatory rabies vaccination and agreed with the statement, “The decision to vaccinate dogs that are kept as pets should be left up to individual pet owners.”
These views were less likely in those with a college education, and more common in those who also held misinformed views about vaccination for children.
A new study has looked at this issue again, in both cat and dog owners.
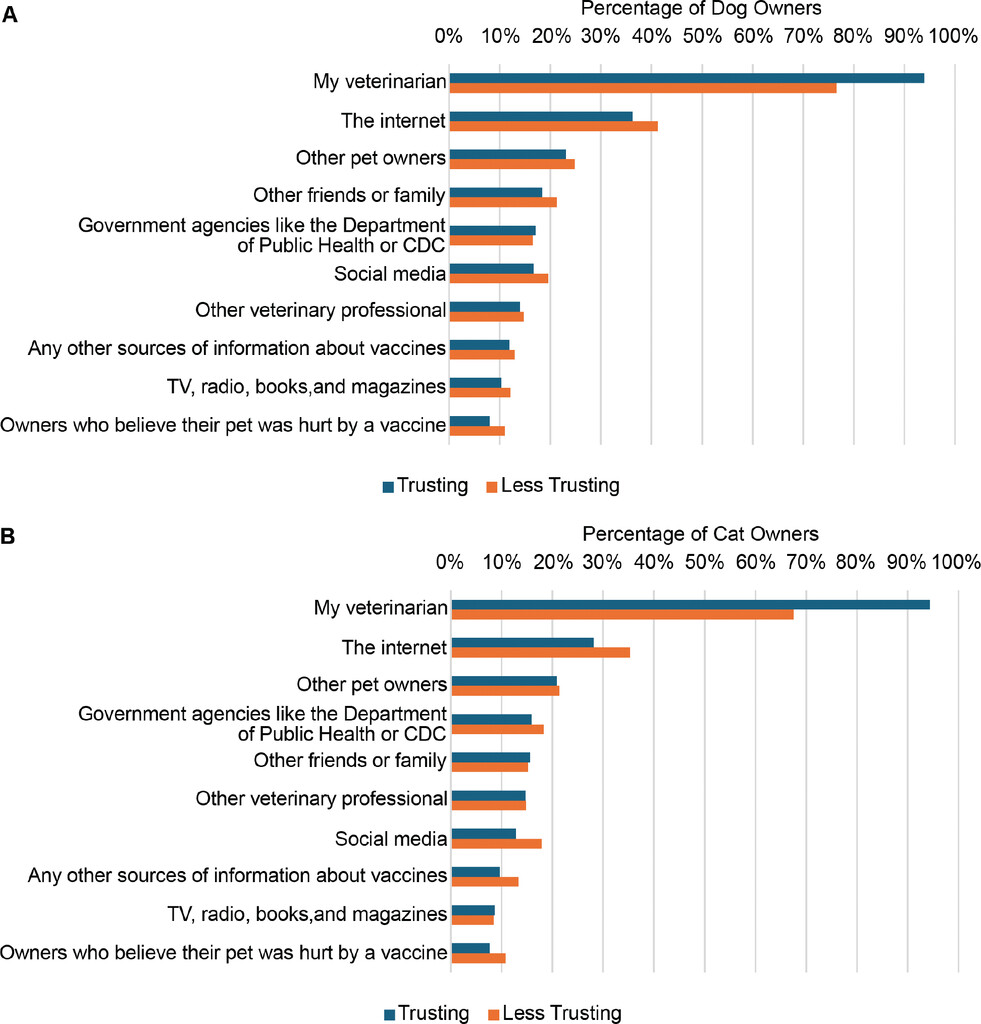
The findings support and amplify messages from previous work, showing that while most pet owners trust their vet and rely on them as the main source of information, all too many are still less trusting and more influenced by less reliable sources of information. The basic findings were these-
Overall, 62.9% of dog and 61.2% of cat owners were classified as trusting their veterinarians.
The longer people know their vets, the more confidence they have in them.
Vets were the primary source of information about vaccines for dog and cat owners, followed by the internet (Figure 1)
Owners with less trust in vets were more likely to turn to other sources, especially the internet, for information.
People who trust their vets are more likely to have their pets properly vaccinated than those who don’t.
Those who rely more on the internet for information are less likely to have their pets properly vaccinated.
Other variables, such as political affiliation and education level, were inconsistently associated with reliance on vets as a primary information source.
This is not a revolutionary study, but one that supports the broad understanding we already have about the role of personal relationships built over time in establishing trust and support clients in making science-based decisions about their pets’ health. It also highlights the unsurprising deleterious role of the internet as a source of information about vaccination (and many other topics!).
In my presentations on mistrust and misinformation, I have emphasized that trust in vets and science remain high overall, though it is eroding among some segments of society. We still have the confidence of many pet owners, and we can still help them protect their pets from the mistakes encouraged by sources of anti-scientific information. But we cannot blindly rely on that confidence, and we must continually nurture the relationships with our clients that allow us to help them resist the rising forces of mistrust and misinformation.
Integrative Medicine- Mixing Apple Pie and Cow Pie A recent issue of the journal Today’s Veterinary Practice contained a couple of articles form some familiar folks who represent the problematic notion of “integrative medicine.” This is a poorly defined term which typically is a way of signaling support for including alternative therapies with little scientific validation alongside legitimate science-based medicine. It creates an aura of open-mindedness and signals that proponent are not extremists but reasonable and willing to use any tool that helps their patients without prejudice. Science-based and alternative therapies are simply tools in a toolbox, and whatever tools suits the job is the one that should be chosen.
This, of course, ignores the fact that we have good reason to believe science-based “tools” actually work, while the safety and effectiveness of alternative methods is often unproven, and sometimes clearly disproven. All therapies should have to meet the same standard of evidence, that of scientific testing, and integrative medicine is simple a way of exempting some treatments from proving their worth objectively.
Mixing treatments that don’t work with those that do isn’t going to improve care. Or, as infectious disease specialist Mark Crislip has put it, “If you mix cow pie with apple pie, it does not make the cow pie taste better; it makes the apple pie worse.”
Nevertheless, the integrative ideology is popular because it feeds into the middle-ground fallacy, the belief that when there are two opposing sides to an issue, the truth is always a compromise somewhere in the middle. In reality, sometimes one side is actually right and the other side is wrong, so eschewing both exclusively scientific and alternative medicine in favor of an integrative mix of the two isn’t necessarily the best path.
Fresh Foods vs Conventional Diets The first article that drew my attention was concerning the possible benefits of “fresh” pet foods. The first author was Dr. Donna Raditic, a nutritionist I have written about a number of times. She was involved in running an integrative medicine fellowship program, and she has been a consistent proponent of mixing alternative therapies, such as herbal medicine, acupuncture, Bach flowers, and homeopathy, with conventional treatments.
The focus of this article is essentially that fresh foods are safer and healthier than “highly processed” conventional diets, due mostly to the concern about potentially carcinogenic chemicals created by “heat processing” (“cooking” to most of us). She advocates using the NOVA classification system, or something like it, to rate pet foods and avoiding those that are highly processed.
I have written in detail about the issue of processing, and the limitations of the concept. While the idea that fresh diets might have some health benefits is a reasonable hypothesis, it is currently supported mostly by associations in observational studies in humans or by lab animal studies that poorly reflect the reality of what people and pets actually eat. Nutritional composition and quality may well be more important for health outcomes, and processing may be a confounder rather than a problem in itself. There is also significant doubt about the value of the NOVA classification system in human nutrition, and about whether using it as a primary guide to the healthiest diet is actually beneficial.
In keeping with the tone of “integrative medicine” thinking, the article contains reasonable hypotheses and raises issues worth considering. However, it presents the benefits of the NOVA system and the risks of processed foods with far more confidence and certainty than is justified by the existing evidence, and it assumes the superiority of the alternatives without any evidence at all. This reveals the underlying bias of the authors, who have clearly already made up their minds regardless of the limitations of the evidence. Assuming the truth of the proposition you are arguing is a type of logical fallacy known as begging the question, and it is prominently displayed in this article.
The authors may, of course, turn out to be right about some of their claims, and if the data showing this appear, I will happily shift my position on fresh diets from neutral to strongly in favor. For now, however, as veterinary professionals and pet owners, we should not obsess about the “processing” involved in the making of the pet foods we use. While inclusion of some fresh or whole foods may well turn out to have some health benefits, it is far more important that making sure our pets are eating complete and balanced diets that meet their nutritional needs, regardless of the form they take.
An Integrative Approach to Aging Regular readers will know that for the last several years I have been deeply involved in canine aging science, working at a company developing drugs to extend healthy lifespan and as part of several scientific collaborations in this area. So I always pay attention to articles and books about aging and longevity.
Unfortunately, there is at least as much hyperbole and outright nonsense in this field as there is legitimate science, and lifespan extension is claimed freely by lots of folks as a benefit for unscientific or unproven treatments that they have long been advocating. I have illustrated this in a number of book reviews, most clear for the book Forever Dog, which is a superficial reframing of many myths and cliches from alternative medicine into an “anti-aging” approach.
Dr. Gary Richter is another of the integrative medicine crowd I have discussed previously, and he has a book on a “holistic” approach to longevity for dogs that I have read but not yet reviewed. Suffice it to say the book contains the usual mixture of reasonable lifestyle advice (maintain a healthy body weight, exercise regularly), mainstream veterinary advice (see a vet regularly, get at least some vaccinations), unproven or exaggerated claims (for unconventional diets and supplements), and outright nonsense (Chinese and other herbal medicine, chiropractic, etc.). Mixing the good, the bad, and the ridiculous may sound enlightened and “open-minded,” but it’s really just cow pie and apple pie again.
In this article, Dr. Richter reviews the hallmarks of aging, a common system used to categorize factors contributing to aging in a way that facilitates study and that might someday be useful as targets for therapies to slow aging. However, as usual there is a lack of any distinction between scientifically validated tools, plausible but unproven hypotheses, and pet theories with no substance or evidence whatsoever. Almost everything is presented equally positively, which makes for an inspiring, but ultimately misleading read.
The real danger of the integrative approach is evident in the fence-straddling Dr. Richter does about vaccination and parasite prevention. He does recommend these as “protect[ing] pets’ immune systems,” but then he almost immediately adds, “inappropriate or overuse of vaccines, antibiotics, and other medications, as well as early spay and neuter surgeries, may have equally impactful negative effects on longevity.” This broad statement is supported by a citation to a paper on the potential risks and benefits of neutering different breeds at different ages, which isn’t really relevant to the doubt he is casting on vaccines or “other medications.”
The reality is that there is zero evidence that recommended vaccination practices constitute “overuse” or have any negative effects on health and longevity. Antibiotic overuse is absolutely a problem in terms of antimicrobial resistance and some effects on the microbiome, but it is not at all evidence that it plays a role in reducing lifespan. And while there are complexities to the issue, the bulk of the evidence in multiple species suggests that neutering increases lifespan. This caveat is fundamentally misleading and creates unnecessary anxiety about beneficial veterinary treatments.
I am all for generating excitement about the potential for new preventive approaches to extending lifespan and healthspan. I think new therapies, from lifestyle changes to drugs and more we haven’t even considered yet, will be available and practical not too far in the future. However, we do no favors to our patients or the longevity field by stoking inappropriate anxiety or unjustified enthusiasm about current practices or those still under investigation. Dr. Richter’s book reads very much like this article, and while it is not as egregiously anti-science as some have reviewed (such as Forever Dog and Nutrigenomics), its strengths are undermined by the credulous and unhelpful “integrative medicine” perspective.
A snippet from a free webinar I co-present with Dr. Lippman and Dr. Tarantino from the Senior and Geriatric Dog Society. You can take the full course here- https://loyal.dog/course-5B-BM