From both my twenty-five years of clinical practice as a general practice vet, and also my work studying aging in dogs, I have developed a particular interest in the care of senior pets. One important aspect of this care is the management of chronic diseases, including palliative care for the symptoms they create, and also the care patients receive at the end of life. While we are fortunate in veterinary medicine to have euthanasia as an option to prevent unnecessary suffering, there is often a period before this point where intensive management of symptoms that can diminish quality of life is needed.
All of us in general practice, and in some specialties, such as oncology and internal medicine, have experience trying to manage such symptoms and support good quality of life in aging pets with chronic or life-limiting illness. However, doing this effectively can take a lot of time and a close relationship with the patients’ human family, and this can be difficult to achieve in the context of routine practice. Many of us have short appointment times (15-30minutes), long wait times for open appointments, and no ability to see the patient at home, where most palliative and end-of-life care takes place. This makes providing the level of such care we feel our patients deserve challenging at times.
One way of meeting this challenge is to work with veterinarians who focus on providing palliative and hospice care, many of whom do so in the patients’ home. These individuals are likely to have additional training and experience, and a context for their practice (often mobile and independent), that can support a higher level of palliative care.
I was intrigued recently when I saw that a group of such veterinarians have begun the process of seeking formal recognition as a medical specialty through the American College of Veterinary Hospice and Palliative Medicine (ACVHPM). This, in turn, has triggered a public comment period, during which anyone interested in the subject is asked to submit an opinion on the proposal to the American Board of Veterinary Specialties (ABVS).
Acceptance as an official specialty acknowledged by the ABVS is an important practical and symbolic step. As I have discussed often in the past, many individuals and organizations claim specialized expertise, and often this is self-serving and misleading to pet owners. Self-designation of specialty status is common in areas of alternative medicine, and it has no value in helping people distinguish safe and effective science-based care from pseudoscience and nonsense. Such fake specialty designations create the false impression of scientific legitimacy where it has not been earned.
In contrast, specialties recognized by the ABVS are generally expected to have a strong foundation in science and rigorous training for diplomates. This doesn’t make any individual or organization perfect or omniscient, of course, but it provides a solid foundation for confidence in the true expertise of specialists and specialty societies. This helps both general practice vets and pet owners recognize reliable sources of information.
I have explicitly opposed applications for ABVS specialty status in the past for both acupuncture and herbal medicinebecause these fields are dominated by pseudoscience and superstition, and specialty recognition would create a false impression of a scientific standard of evidence and training that the fields do not actually have. This would mislead rather than help primary care vets and owners.
I have been supportive of most other specialty designations, though I admit to a bit of ambivalence about the status of the American College of Sports Medicine and Rehabilitation (ACVSMR). Physical therapy (typically called “rehabilitation” in U.S. veterinary medicine for legal reasons) is an important and generally science-based field in human medicine, and I strongly support its development for veterinary patients. Managing and maintaining physical activity and function and dealing with chronic pain and musculoskeletal disease is critical for wellbeing in senior patients in particular, and we do far too little of this.
As the field is quite new, there is understandably limited evidence for most specific interventions. This is a deficit that will hopefully be remedied with time and effort, and having a specialty college can support the necessary research. However, the lack of evidence also means many working in this field are accustomed to and comfortable with limited evidence, and they may naturally turn to anecdote, personal experience, and theoretical reasoning to support specific treatment choices, even those these are often unreliable evidence. My experience is that questionable or likely ineffective treatments, such as acupuncture, chiropractic, cold laser, and others I have evaluated repeatedly, are quite common in the rehabilitation field, possible due to the high level of comfort with low-quality sources of evidence.
This is problematic not only because patients may be exposed to ineffective treatments but also because the use and endorsement of these treatments by recognized specialists lends them a validity that the scientific evidence does not support. I do worry that this will lead to these therapies becoming entrenched in the discipline and actually impede research on them or the abandonment of treatments when the evidence warrants it.
So when I heard about the ACVHP petition, I was similarly ambivalent. I have written here many times about hospice and palliative care, and the tension between our need for more and better care of this kind and the deep entrenchment of dubious and pseudoscientific therapies in the field. The leading organizations and individuals in the field explicitly endorse therapies with questionable supporting evidence (e.g. herbal remedies and acupuncture) and those which are clearly only placebos (e.g. homeopathy and “energy” therapies) alongside science-based medical practices.
As much as I admire the vets who do this kind of work, I feel very strongly that providing ineffective and unscientific therapies are not in the best interests of patients, and they can cause real harm, both directly and indirectly. Having members of a recognized mainstream specialty offering such therapies would create the same kind of false impression of legitimacy seen with questionable treatments used by rehabilitation specialists.
I know there are members of the hospice and palliative care community committed to science-based medicine, and several have reached out to me over the years expressing their frustration with the prevalence of alternative and unscientific practices in their field. The question raised by the ACVHP proposal is whether building and recognizing a specialty would increase the standards of scientific evidence for interventions used in the field and squeeze out the bogus and questionable practices or simply legitimize and sustain them.
I can’t honestly predict which possible outcome is true. My experience with the ACVSMR so far in its relatively short existence has been mixed. The increased attention to rehabilitation has been a positive force, and there is a growing body of research to develop more evidence-based therapies. However, the questionable practices often used in this field are also growing in popularity in many cases, and it does seem that the endorsement of specialists for these practices makes it harder to explain the scientific case against them and convince regular vets that they are better off not adopting or recommending these practices.
Ultimately, I feel like the prevalence of questionable practices in the hospice and palliative care field is too high. Research is especially challenging to do in this population and setting, which adds a further barrier to building a better evidence base and pushing out ineffective treatments. I don’t believe specialty status is warranted based on the existing level of scientific evidence, and I am not confident that having a recognized specialty will improve the evidence and the quality of care. I fear it will simply sustain and entrench the practices favored by the most persuasive voices in the field, leading to standards set by personal opinion rather than science.
Based on this concern, I submitted the following comment to the ABVS in opposition to the proposed specialty-
I must oppose this position, with reluctance. I think expanded and high-quality palliative and hospice care for veterinary patients is much needed. Unfortunately, the IAAHPC and many of its leaders and members explicitly support the use of implausible and disproven alternative therapies in hospice and palliative care patients. Homeopathy, Reiki, TCVM acupuncture, and other such alternative methods lacking scientific validation don’t benefit our patients. Providing them with, or even in lieu of, science-based medicine harms patients and misleads clients. Board specialty status would be more likely to legitimize such therapies than replace them with evidence-based medicine, so I must oppose granting this status.
I remain cautiously hopeful that the voices in this field advocating for an evidence-based approach will grow stronger and more influential, and that the field will move towards a more science-based approach. Unlike acupuncture, which has had more than a fair chance to prove itself and has failed consistently, I believe robust and science-based hospice and palliative care is a necessity in veterinary medicine, and I would like to see this develop to the point where a specialty is warranted and can be a positive force for the advancement of the field.
I was privileged to be asked to speak at this event on the subject of using biomarkers to support a more proactive, preventative approach to pet health.
Below you can find the recording of this session as well as the more detailed proceedings summary
I gave the opening plenary at this conference on the subject of Healthy aging, and also did a deep dive into potential measures of biological age. Enjoy!
“Nutritionist” isn’t a protected term. Anyone can call themselves a nutritionist. “Dietician” is the legally protected term. “Dietician” is like “dentist”, and “nutritionist” is like “tooth-i-ologist.” Dara O’Biain
In one of the most insightful and frighteningly prescient books I’ve read, The Death of Expertise, Tom Nichols makes the case that the value of credentials and legitimate specialized knowledge have declined due, in part, to cultural resentment against “elites” and a general sense that belief is more important than knowledge, that everybody’s view of reality has an equal right to be taken seriously. The catastrophic stupidity now crippling science and public health in America certainly seems to prove his point.
However, in a weird contradiction, promoters of pseudoscience and unproven or ineffective approaches to health have also always longed for the legitimacy, and marketing advantage, that comes with credentials and the appearance of expertise. Acupuncturists and herbalists have repeatedly sought recognition as recognized specialties in veterinary medicine. They crave the respect that would come with such recognition, and they know that it would help them sell their services to more people.
If unable to earn such recognition from mainstream, science-based sources, organizations and individuals often create their own organizations to recognize themselves. You can get a certification not only in dubious areas of medicine, such as homeopathy and chiropractic, but even as a psychic or an astrologer. In seeking the legitimacy that comes with real credentials but creating fake ones, proponents of such practices deceive the public and devalue real expertise.
A reader recently asked me to look into the claims and credentials of one of many online sources of advice about nutrition for dogs and cats, Kimberly Lloyd from The Holistic Canine. This proved to be an interested example of the tension between disdaining mainstream scientific opinion and yet wishing to promote one’s advice as scientific, even evidence-based expertise.
Lloyd offers advice and consulting services around nutrition for dogs and cats as well as “Natural health care” and “therapeutic health care,” which are claims probably vague enough to avoid the letter, if not the spirit of the laws against practicing veterinary medicine without a license. She also has a business providing nutrition and health advice for humans, proving that apparently it is possible to be an expert in everything.
The advice she gives, as is often the case among proponents of alternative approaches to nutrition, is a mix of reasonable and ridiculous. Encouraging people to keep their pets at a healthy weight is a sensible and obvious bit of advice, for example. She talks a lot about fresh-cooked foods, which I am quite optimistic about (though the true health value of these compared to traditional formulations still hasn’t been demonstrated scientifically.) Overall, there is plenty of ordinary, reasonable advice on her page. It is by no means the worst I have seen!
Unfortunately, there is also plenty of information that is misleading or pure pseudoscience:
She advocates raw diets, despite the lack of a coherent theory or any meaningful evidence they are beneficial and the real risk of infectious and parasitic diseases from eating raw meat.
She makes lots of claims about the value of specific herbs that are entirely belief based, with no convincing scientific support.
She has called commercial pet food, “ the single greatest disservice to our pets,” which is nonsense.
She also disdains much of science-based medicine, saying that’s second to commercial diets the greatest disservice to our pets is “unnecessary conventional veterinary practices and interventions” and “chemical ‘preventatives.’”
Like many proponents of raw foods, she seems to be a vitalist, believing in some magical “energetic” properties to foods- “food goes far beyond physical matter.” She dresses up her vitalism in a coat of pseudoscientific paint with lots of references to “microRNA,” but her rant against “chemical-laden, vaccine-poisoned, antibiotic-polluted” ingredients, and her discussion of the role of “energy” and belief in managing cancer reveals her perspective as incompatible with science.
She claims to be able to interpret clinical lab test results–“At The Holistic Canine, we interpret labs based on the big picture. If you’d like help understanding your dog’s results, we are only a phone call away!” This is well within the practice of veterinary medicine and isn’t appropriate for someone without appropriate training in clinical pathology and a license to practice veterinary medicine.
She denigrates commercial therapeutic diets, despite the robust scientific evidence for their benefits, and promotes herself as capable of formulating better alternatives—“ The Holistic Canine creates custom therapeutic diet formulations designed specifically for pets with medical conditions. Each plan is carefully structured to meet nutritional requirements while supporting the individual needs of the animal.” Again, this is only appropriate for a true board-certified veterinary nutritionist or someone with a doctorate in clinical nutrition form an accredited institution.
She proudly asserts that she does not vaccinate her own children and lists herself as “as strong voice against vaccination.” This alone should realistically disqualify anyone from given health advice.
Of course, anyone is free to set up a web site and offer their opinions on healthcare. Charging for these opinions is a bit more ethically problematic, particularly when they conflict with established science-based healthcare, but this is certainly common these days. The question here is what credentials does the person giving the advice claim, and what do these mean. This is a bit of a challenge since many titles and credentials are offered in various places, and the sources and details about them are not usually provided (itself a bit of a red flag).
The advice on this site is promoted as “evidence-based,” (which it absolutely is not) and as coming from a legitimate credentialed expert, with labels like “board-certified nutrition practitioner,” “canine and feline clinical nutritionist,” “certified raw dog food nutritionist,” and others as well as claims to offer “clinical” and “therapeutic” nutrition counseling. So what can we determine about the credentials being promoted here?**
PhD in Holistic Nutrition and Naturopathy
While a PhD in nutrition can be a legitimate credential for a veterinary nutrition specialist, this credential does not appear to be of that sort. Her Facebook page suggests this degree comes from an unaccredited online school, the University of Natural Health, which offers none of the rigor or science-based content of a legitimate doctoral degree in nutrition. (Elsewhere, she lists her affiliation as the College of Natural Health” or the “Natural Health College,” so it is not completely clear this is the institution she obtained her credential from). At the University of Natural Health, this degree requires a 3,000 word paper “on a specific aspect of natural health, as applied in his or her own life and/or in the lives of others.” This is nothing like the research-based process of completing a meaningful doctoral degree in nutrition.
BS in Nutrition
This is listed as a credential in several places, but the institution is not named. It is unclear, therefore, if this is a legitimate degree from an accredited university, but of course even if it is, this does not qualify her as a “clinical” or “board-certified” veterinary nutrition specialist.
Board-certified Holistic Health Practitioner
This is a credential from the American Association of Drugless Practitioners (AADP). This group, like organizations credentialling homeopaths and Reiki practitioners, is a classic example of a fake institution set up by practitioners of unscientific alternative therapies to generate the perception of legitimacy. It is not accredited or recognized by any mainstream, science-based organization, such as the American Board of Medical Specialties.
The same is true for the other organizations she cites as validating her education-the International Practitioners of Holistic Medicine (IPHM) and the International Institute for Complementary Therapists (IICT). These are both membership organizations of people promoting alternative therapies and not accredited or recognized by any mainstream, science-based bodies. They exist, like the AADP, in an alternative institutional universe to validate themselves and their members since the accepted organizations of science and medicine do not accept their claims or practices.
Certified Canine and Feline Nutritionist
The educational content behind this online program from Southern Illinois University is RACE approved, and it is scientifically legitimate. The program technically offers a “Certificate in Canine and Feline Nutrition,” a subtle difference in wording that avoids the impression given on the Holistic Canine web site that it confers some kind of specialty status.
While the content is approved for continuing education credits for vets and veterinary technicians through the American Association of Veterinary State Boards (AAVSB), completing it does not make anyone a “board-certified” nutritionist. And while the information may be useful for anyone, the continuing education credits only apply to people with a state license as a veterinarian or veterinary technician, which is not the case here.
While I applaud anyone who puts the time and effort into getting additional education like this about nutrition, the content on the Holistic Canine web site and social media make it clear that the science-based information taught in this course is routinely ignored, and the purpose of the certificate is only to create the impression of scientific legitimacy for pseudoscientific advice.
Certified Canine Raw Food Nutritionist
This is not a real thing. Again, the granting institution is not specified, but the alternative publication Dogs Naturally Magazine offers an online course that may be what is referred to here. A few other sources offer training in raw feeding, but since this is not a scientifically validated practice, such certification does not imply science-based expertise.
A variety of other credentials are offered, including “certified Natural Health Practitioner (CNHP) and Holistic Nutrition Practitioner (CHNP).” Again, no institution is specified, but there are no legitimately accredited educational institutions that offer such credentials, so these likely come from the same or similar elements of the self-referential ecosystem of alternative institutions and credentialing bodies.
Finally, the site mentions a Master’s of Divinity, again without specifying the institution (some Facebook posts suggest this is from another unaccredited, online institution, but I could not confirm this). This is not directly relevant to her purported expertise in veterinary nutrition, but she does reference it when teaching courses for humans that mix health, lifestyle, and spiritual advice,
The point here is that advocates of alternative health practices, whether nutrition-centered or others, tend to want to have their cake and eat it too. They frequently condemn mainstream scientific institutions and those with expertise derived from them. At the same time, they understand that pet owners respect expertise and want to get advice from people who have the appropriate background to know what they are talking about. Their response is often to construct alternative institutions and credentials to give the appearance of scientific legitimacy to ideas and practices that are ultimately cannot meet the standards of evidence required by mainstream science.
It is easy to mislead pet owners into believing that there is a serious difference in scientific opinion or uncertainty in the scientific evidence when really there is not. There is legitimate expertise, such as obtaining board certification through the American College of Veterinary Internal Medicine or the equivalent in Europe or elsewhere, and there is fake expertise, including most of the credentials and titles claimed by Kimberly Lloyd.
All of the claims of being “scientific” in her recommendations, even when they are not based on any actual scientific evidence or are directly contradictory to such evidence, are misleading and disingenuous. Adding a host of alternative titles and degrees does not fix this. Pet owners are free, of course, to follow alternative approaches to health and nutrition, but they should make this choice with a full and clear understanding that these approaches are not supported by science and that the “experts” promoting them are only experts by their own judgement.
**I have attempted to identify and verify the credentials claimed publicly by Kimberly Lloyd as best I can. The specific programs and institutions granting these are not always listed anywhere obvious, and my conclusions about some may be in error. If evidence of errors appears, I will of course post appropriate corrections.
Several times in the past, I have written about he potential usefulness of cranberry extract in various forms for treating or preventing urinary tract infections (UTI) in dogs and cats. The last time I covered the subject was way back in 2017, and the evidence was still not conclusive, in veterinary patients or humans:
There is weak theoretical justification for using cranberry products for UTIs, though none of the supporting preclinical evidence involves dogs or cats. There is conflicting clinical trial evidence in humans, and no clinical studies in dogs and cats.
This [Cochrane] review indicates pretty clearly that overall, cranberry juice is not effective in preventing UTIs despite theoretical reasons why it might be. This illustrates, yet again, why we cannot rely on extrapolation from pre-clinical or in vitro studies to tell us what will work in actual patients.
The in vitro portion of this study is consistent with existing research that suggests cranberry extracts may reduce the ability of some bacteria to stick to the lining of the urinary tract. This could theoretically help prevent some urinary tract infections, though clinical research in human patients suggests this doesn’t really work to a significant extent in living people.
The portion of the study looking at prevention of UTIs in actual dogs, unfortunately, doesn’t help establish what benefit, if any, this product might have.
Despite some promising laboratory studies suggesting cranberry supplements might help prevent or treat urinary tract infections, the evidence of studies in clinical patients has been disappointing. Conflicting studies in humans suggest, on balance, that there is probably no significant benefit. And now a high-quality clinical trial in dogs has failed to find any effect, even in the the of infections the pre-clinical research most strongly suggested there should be one.
While the risks of cranberry supplements are probably negligible, pet owners should understand, and veterinarians should make in clear to their clients, that there is no good reason to believe they have any real value in preventing or treating urinary tract infections.
Here we are nine years later. Surely, the question must have been answered definitively by now? Yeah, about that…
A recent systematic review evaluated the research evidence to date on the topic.
Limited data are available regarding the use of cranberry or cranberry extracts for the prevention or treatment of infectious urinary tract disease in dogs and cats…While indirect evidence from humans and in vitro data from dogs and cats suggests the potential for efficacy, the small number of studies, small sample sizes within those studies, and low certainty of evidence preclude confident assessment of the role of cranberry for the prevention or treatment of infectious urinary tract disease in dogs and cats.
Despite decades of claims, research, and clinical use in patients, we still can’t say with any confidence whether or not cranberry, in whatever dose and form, is at all useful.
This is a common situation in veterinary medicine, where resource limitations and cultural factors rarely allow for large-scale, robust scientific evidence to answer such questions with confidence. However, in this case, the greater resources and efforts made in humans haven’t proven a whole lot better.
Cranberry juice reduced the rate of UTIs about 27% compared with a placebo liquid and appeared to improve symptoms somewhat.
Cranberry juice also appeared to reduce the use of antibiotics by about half compared with a placebo liquid.
Other forms of cranberry supplement didn’t seem to be helpful.
The evidence for benefit was only moderately certain.
Another recent review found similar benefits, but not for certain groups, including elderly people in institutions and people with neurological conditions impairing their urination.
Bottom Line The inconclusive nature of the veterinary research, and the caveats and nuances of the human literature, make it effectively impossible to say whether any form of cranberry supplement will benefit individual dogs or cats at risk for UTI. There is no evidence for significant safety concerns, and if using these products reduces excessive or inappropriate antibiotic use in patients with urinary tract disease, that might be an indirect benefit. Still, it is frustrating that we still cannot have confidence in the effects of these products, and should remain skeptical of the claims made for them by manufacturers and others with opinions based on anecdotal evidence.
I was recently asked about a specific acupuncture technique which pops up from time to time– needling or injecting medications at the location known as GV20 for calming or sedating effects.
It is always problematic to evaluate specific claims in acupuncture because-
Almost no one understands this, and acupuncturists have invented many complex and scientific-sounding ad hoc explanations for how acupuncture is supposed to work. These explanations are typically unproven, and while they explain some of the effects of needling and electrostimulation (and any other minor local trauma), they don’t support the broad, system effects proponents claim for acupuncture
Almost no one understands this, and acupuncturists are always identifying special characteristics for particular locations they claim as treatment points. Unfortunately, you can find something “special” (nerves, blood vessels, tendons, etc.) at nearly every point on the body, but again there is no convincing, consistent evidence that the collection of locations used for acupuncture is real.
There are many clinical studies of acupuncture treatment. Some look like they show meaningful benefits. This is mostly an illusion made out of placebo effects, bias and error in study design and reporting, tooth-fairy science, and minor non-specific effects from sticking needles in things. The bottom line is that acupuncture is mostly placebo, non-specific local effects of minor trauma, and the effects of other interventions credited to acupuncture.
Almost no one understands this, and the sheer size of the acupuncture literature is enough to convince a lot of people despite the fatal flaws in it.
All of this makes any attempt to challenge claims about specific acupuncture treatments challenging, and probably pointless. A thorough critical evaluation of studies around the use of GV20 is arguably meaningless if GV20 doesn’t exist and no one who believes in acupuncture will change their mind no matter what the results are. Despite that, shouting science into the void is arguably a majority of the content of this blog, so here goes….
What is GV20? The short answer is that it is an imaginary construct that acupuncturists claim as a functional and anatomically specific treatment location.
Traditionally, the governing vessel has been said to “connect all yang vessels in the body and functions to regulate local qi and blood, and modulate the balance between yin and yang”1 as well as to regulate “liver fire” and “internal wind.” This, of course, is all meaningless nonsense, but despite claims to the contrary it is how this and other acupuncture treatments are determined. Attempts to find “scientific” explanations for specific points and how they work are all post hoc rationalizations for a system still founded in this kind of pseudo-religious folk mythology.
Consistent with the general trend in acupuncture to look in an area that pre-scientific folk medicine claims is special and then report whatever is found there to be the reason for why the location is special and therapeutically relevant, many papers have characterized the anatomic and physiologic features of location of “Governing Vessel 20” or “Baihui.” It has been identified by anatomic landmarks relative to the skull, ears, or hairline, the purported presence of cranial or peripheral nerves, the presence of connective tissue, proximity to the central or precentral sulcus of the frontal lobe, and other criteria.1–4 Somewhat circularly, it has also been identified in terms of the supposed clinical effects of doing acupuncture there.
The purported uses for acupuncture at GV20 include3,d brain and bone marrow disorders, palpitation, stroke, loss of consciousness, chronic or acute infantile convulsion, sunstroke, irregular menstruation due to deficiency and cold in the lower jiao, dysmenorrhea…brain
disorder and mental disorder, such as heaviness of head, dizziness., vertigo, manic-depressive disorder, epilepsy, palpitation and poor memory; headache, dizziness, eye pain and redness, irritability, hypertension, anal, uterine, and vaginal prolapse and hemorrhoids; nasal obstruction and allergic rhinitis and insomnia.
This broad list is typical of claims for acupuncture, and other folk medicine traditions, which are often a hodgepodge of unrelated symptoms and conditions reflecting the foundations of these methods in vague theory and the accumulation of trial-and-error anecdotes. Most commonly, GV20 is used with the intention of sedating or calming pets for veterinary treatment, including potentially to reduce the dosage needed for sedative and anesthetic drugs.
While this sounds like a worthy goal, given that such drugs do have risks and unwanted effects, it is critical to establish that this treatment actually works and doesn’t have its own unwanted effects before using it as a substitute for well-established and thoroughly studies science-based treatments. We do not benefit our patients by believing we have made them more comfortable and withholding necessary drugs if that belief is false.
GV20 and the Evidence Acupuncture research inevitably raises the issue of Tooth Fairy Science. It is possible to generate extensive and impressive data and statistics evaluating imaginary treatments, and these data mislead rather than enlighten us. If Qi and Yin/Yang and meridians and points don’t exist, if they are just folk medicine metaphors unconnected with physiological reality, then clinical trials studying them can never give us reliable evidence about the value of treating them.
Acupuncture, of course, is an especially challenging practice to tests scientifically. While the folk-medicine theories behind it are nonsense, sticking needles in tissue actually does something, and it is fair to ask whether this something might have some value anyway. However, studies of acupuncture are nearly always designed, conducted, and analyzed by people who believe deeply in the power of acupuncture, so the potential for bias to influence the results is pretty great. This is seen in the consistently unreliable data about acupuncture coming from countries with a cultural bias in favor of the practice.5–9
Of course, clinical research incorporates multiple methods for mitigating the impact of such bias, and these can be helpful. Some of them, unfortunately, are very difficult to use in acupuncture studies. Blinding, for example, is difficult to achieve with patients (who can often tell if they are really being stuck with needles or not), and it is impossible to achieve for therapists, who will always know whether they are giving “real” acupuncture treatment or a sham. Since it the demeanor of the therapist can have a significant impact on the patient’s perception of their condition, it can be difficult to trust seemingly positive results from such studies, especially when the outcome measure is something very subjective like pain, nausea, etc.
That said, we do the best we can with the evidence we have, so let’s take a look at an example of the type of research cited to support using acupuncture at GV20.
One study involved giving the common sedative dexmedetomidine, and its reversal agent, under the skin (SQ) at the GV20 location compared with giving these drugs by other routes and in other locations for the purposes of sedating dogs for x-rays.10 This is sometimes called “pharmacoacupuncture,” which seems a bit of a bait-and-switch.
Dogs were randomly assigned to get the sedative, and the reversal agent, in a vein IV), a muscle IM), or under the skin (SQ) at the GV20 point. Sedation was measured by numerous techniques and lots of comparisons were made between the various injection locations.
There were many statistical tests done, most showing no difference form chance and some appearing to. The most consistent finding was that sedation given into a muscle was slower and less effective than sedation given into a vein. Sedation at GV20 appeared to be intermediate between the two, and generally more like IV than IM administration.
The differences were sometimes statistically significant but it is not clear that they were clinically meaningful. The goal (taking orthopedic x-rays) was achievable for all groups, and the adverse effects were minor and not different between the IM and SQ groups (they were greater for the IV group, though none were serious or a reason not to give the sedative by this route if needed).
So what does this have to do with acupuncture? Not much, honestly.
The authors themselves point out that no sedative was given at a SQ spot on the head, or anywhere else, that wasn’t deemed an “acupuncture point.” Perhaps the differences had to do with giving the drug under the skin compared to in a vein or muscle. Or perhaps the head has a particularly good blood supply (scalp wounds are notorious for bleeding profusely), so drugs given SQ here absorb well. There is, in fact, another study comparing administration of sedatives at GV20 and another SQ spot on the head that found not meaningful difference between the locations, so this is quite likely the case.11
There are many plausible explanations for the findings that have nothing to do with the theoretical rationale for acupuncture or the issue of whether or not it works as a general approach. This study doesn’t even convincingly justify the supposed effects of needle stimulation at GV20, much less the larger practice of acupuncture.
Bottom Line Nearly all the studies purporting to validate the benefits of acupuncture at GV20 use injections of drugs or electrical simulation, and none that I have seen effectively control for bias while comparing needling alone at this spot to an appropriate control. Given the implausibility of the traditional explanations for acupuncture, the lack of consistent and convincing evidence that “acupuncture points” exist as a discrete, consistent, identifiable functional entity, and the lack of solid scientific evidence to support the specific claims made about GV20, it is not appropriate to rely on needling at this point as primary component of sedation or pain control for dogs.
As I have said in the past, acupuncture is pretty low-risk in itself, and most of the danger associated with it lies in substituting an ineffective practice for treatments that actually work. If vets want to stick a needle in the head while they also give appropriate science-based treatments for pain, anxiety, and sedation, this is unlikely to do any direct harm. But the belief that this is an “ancient,” Powerful,” or “proven” treatment method is unjustified, and it can lead to unnecessary suffering if we rely on it in place of therapies with better supporting scientific evidence.
References 1. Yang Y, Deng P, Si Y, Xu H, Zhang J, Sun H. Acupuncture at GV20 and ST36 Improves the Recovery of Behavioral Activity in Rats Subjected to Cerebral Ischemia/Reperfusion Injury. Front Behav Neurosci. 2022;16. doi:10.3389/fnbeh.2022.909512
2. Shen EY, Chen FJ, Chen YY, Lin MF. Locating the Acupoint Baihui (GV20) Beneath the Cerebral Cortex with MRI Reconstructed 3D Neuroimages. Evid-Based Complement Altern Med ECAM. 2011;2011:362494. doi:10.1093/ecam/neq047
3. Qian L, Jiang Y, Lin F. Mechanism of the acupoints of the governor vessel in treatment of post-stroke depression on the base of the specificity of meridian points. World J Acupunct – Moxibustion. 2019;29(3):244-248. doi:10.1016/j.wjam.2019.07.004
4. Martha A. Littlefield DVM MS. Anatomic Review of Ten Important Canine Acupuncture Points Located on the Head: Part I. Am J Tradit Chin Vet Med. 2019;14(2):55-66.
5. Wang Y, Wang L, Chai Q, Liu J. Positive Results in Randomized Controlled Trials on Acupuncture Published in Chinese Journals: A Systematic Literature Review. J Altern Complement Med. 2014;20(5):A129-A129. doi:10.1089/acm.2014.5346.abstract
6. Vickers A, Goyal N, Harland R, Rees R. Do certain countries produce only positive results? A systematic review of controlled trials. Control Clin Trials. 1998;19(2):159-166. doi:10.1016/s0197-2456(97)00150-5
7. Masuyama S, Yamashita H. Trends and quality of randomized controlled trials on acupuncture conducted in Japan by decade from the 1960s to the 2010s: a systematic review. BMC Complement Med Ther. 2023;23:91. doi:10.1186/s12906-023-03910-3
8. Ma B, Qi G qing, Lin X ting, Wang T, Chen Z min, Yang K hu. Epidemiology, Quality, and Reporting Characteristics of Systematic Reviews of Acupuncture Interventions Published in Chinese Journals. J Altern Complement Med. 2012;18(9):813-817. doi:10.1089/acm.2011.0274
9. Li J, Hui X, Yao L, et al. The relationship of publication language, study population, risk of bias, and treatment effects in acupuncture related systematic reviews: a meta-epidemiologic study. BMC Med Res Methodol. 2023;23:96. doi:10.1186/s12874-023-01904-w
10. Leriquier C, Freire M, Llido M, et al. Comparison of sedation with dexmedetomidine/atipamezole administered subcutaneously at GV20 acupuncture point with usual routes of administration in dogs presented for orthopaedic radiographs. J Small Anim Pract. 2023;64(12):759-768. doi:10.1111/jsap.13668
11. Llido M, Leriquier C, Juette T, Benito J, Freire M. Comparison of sedation with dexmedetomidine administered subcutaneously at 2 different locations on the head in dogs. Can Vet J. 2024;65(4):351-358.
Why ask the question? The question implies a conflict, a potential incompatibility. If this doesn’t actually exist, then the subject is moot and we can all go home early.
Proponents of complementary and alternative veterinary medicine (CAVM- also labeled “holistic,” “integrative,” “natural,” and many other terms we will explore shortly) typically claim that science and evidence support their practices. They recognize the marketing value of science, and they often assert that the conflict is a mere misunderstanding, or the result of ignorance, prejudice, or avarice rather than a true conflict between their approach and that of science-based medicine.
For example, the online College of Integrative Veterinary Therapies advertises its curriculum as “a wide range of evidence-based courses…bridging cutting edge science and tradition.”1 A prominent proponent of so-called Traditional Chinese Medicine claims that integrative medicine “provide[s] comprehensive, evidence-based care that integrates the best of conventional and complementary approaches for the well-being of animal patients.”2 You can read journals like Evidence-based Complementary and Alternative Medicine, or articles reporting clinical trials evaluating Reiki, “a biofield therapy currently used in hospitals worldwide [with] scientific evidence [that] supports its effectiveness in addressing many physical and emotional conditions.”3 Even the World Health Organization states that “Evidence-based complementary medicine has the potential to support mainstream medicine and more comprehensively support people’s health and well-being needs.”4
So what’s the problem? Why ask the question at all? Well, the problem is that despite both honest and disingenuous efforts to coopt the language of science and EBM, most of what we typically label CAVM is founded in beliefs and models of nature incompatible with a scientific understanding, and these practices are validated almost entirely by faith, personal experience, cultural tradition, and poor-quality efforts to mimic rigorous scientific investigation. EBM is more than a collection of jargon; it is an approach to knowledge that conflicts directly and forcefully with the philosophy underlying much of CAVM.
Sometimes this divide can be bridged and truly scientific evaluation of CAVM methods can be undertaken. When this happens, the results mostly show these methods don’t work. In the rare cases where they do, they can, and should, simply become part of medicine, stripped of their mystical folk belief systems. In the words of two former editors of the New England Journal of Medicine,
“There cannot be two kinds of medicine—conventional and alternative. There is only medicine that has been adequately tested and medicine that has not, medicine that works and medicine that may or may not work. Once a treatment has been tested rigorously, it no longer matters whether it was considered alternative at the outset. If it is found to be reasonably safe and effective, it will be accepted.”5
It is instructive to note, though, that proponents of CAVM often object to this type of deep acceptance, arguing it strips away the very core of what make their methods valuable. This illustrates the depth of philosophical incompatibility between science and most of CAVM. As these defenders put it:
“Any CAM practiced its original way cannot be the same as its biomedical version.…If the biomedical paradigm is adopted, the system will have the characteristics of that paradigm- materialistic, mechanistic, reductionistic, linear-causal, and deterministic.”6
“Scientifically constructed ‘evidence’ for an alternative therapy only works when the therapy has mutated into a medicalized version and divested itself of its alternative philosophy. The very publication of trials can act as a reformulation of the very nature of a therapy, generally in the direction of medicalization.”7
The only reason CAVM exists as a category, then, is to highlight the special origins of certain practices as different from those accepted in science-based medicine. This serves both a marketing purpose (selling treatment that is “special” and “different” from conventional medicine) and also as an excuse for utilizing treatments without the type and level of evidence expected for mainstream medicine.
Doctors who would never prescribe a new antibiotic with undisclosed ingredients and no clinical trial data showing safety or efficacy, one that is purported to kill bacteria by targeting its “energy signature,” will happily prescribe herbal or homeopathic remedies with no better evidence. The labels of “natural” or “traditional” are used as excuses to imply safety and effectiveness and evade the normal standards of evidence.
“By definition…complementary and alternative medicine…has either not been proved to work or been proved not to work. Do you know what they call alternative medicine that’s been proved to work? Medicine. Tim Minchin”8
What is CAVM? Before I go further, I should try to define CAVM. This is harder than it sounds because the term encompasses a variety of approaches that conflict with science-based medicine in different ways, to different degrees, and that often conflict just as much with each other. The unity, such as it is, lies not in any shared understanding of nature or of how medical therapies should be validated, though there is some broad agreement on elements of these. The real bond that connects CAVM approaches is their status as “other,” defined in opposition to science-based medicine.
This opposition may be based on conflicting views of nature, competing cultural traditions, or simple part of a promotional strategy to distinguish oneself and one’s practices from other vets and what they offer. The “alternative” in CAVM was the original term for this loose collection of approaches, and it was meant to designate a replacement for conventional, science-based medicine. That proved too much for most human patients, and for most animal owners, who were mostly unwilling to abandon the obviously successful approach that brought us vaccination, antibiotics, and emergency rooms.
This led to the adoption of the term “complementary,” suggesting it was beneficial to use unscientific or unproven practices alongside science-based medicine. This has been more successful, but proponents of CAVM dislike the implication that what they offer is an afterthought or second-rate compared with conventional medicine. This has led to the most successful label; “integrative medicine.”
The idea behind this label is that scientific and alternative therapies are different but equally useful tools available to veterinarians, and each should be used when appropriate without any distinctions based on their underlying theoretical rationales or history. The term suggests we can seamlessly blend alternative and conventional therapies, that they are equally useful and reliable tools we can select from for the medical job at hand.
However, this obscures the reality that there are important practical and philosophical differences between how alternative and conventional therapies are developed, tested, and employed, and these differences matter. Integrative implausible, unproven, or demonstrably ineffective therapies with scientifically validated treatments adds no benefit for the patient, and it can even do harm.
As infectious disease specialist Mark Crislip has put it, somewhat scatologically, “If you mix cow pie with apple pie, it does not make the cow pie taste better; it makes the apple pie worse.” (for those not familiar with the English idiom “cow pie,” it refers to bovine feces)
The Conflict: Philosophy The core conflict here is philosophical. In terms of epistemology (the science of how we know things), proponents of CAVM largely reject the diagnosis of the disease EBM, and science generally, exists to treat. Forms of evidence viewed as weak and unreliable by EBM are privileged in CAVM, and those types of evidence higher on the pyramid are seen, at best, as nice to have but fundamentally unnecessary to support a given clinical practice. At worst, they reject the very idea that such evidence is more accurate or reliable than personal observation, anecdote, tradition, or pure faith. Science often serves only a marketing function in CAVM, not a meaningful role in choosing and rejecting ideas and practices.
Philosophically, CAVM relies predominantly on trust in personal belief and observation, and in the historical beliefs of individuals or previous generations of folk medicine practitioners. The most extreme proponents reject the hierarchy of evidence behind EBM entirely:
“[EBM] buttresses the idea that there is a legitimate hierarchy of knowledge and method with the [randomized control trial] as the gold standard and the clinician’s notes, observations, and judgments right down there in status with ethnography, sociology and anecdote…there are practitioners of naturopathic modalities who do not subscribe to this hierarchy at all”9
“For ancient and traditional healing modalities, one could argue that history provides the evidence on which to base clinical practice…One cannot conclude that, because a healing system cannot be measured conventionally, it is ineffective or unsafe.”10
“Users of homeopathy did not see a need for scientific testing and were happy with their own judgment of whether the treatment was working for them…[Randomized clinical trials] came at the bottom of their hierarchy of evidence.”7
“The invocation of a saint can cure intractable cancer; a voodoo curse can kill.… A shaman applying a curse does not consider it to be a placebo, nor does his victim. To them, real magic is involved…We can never prove the shaman wrong, only offer an alternative explanation.”6
“As a veterinarian now practicing homeopathy and chiropractic almost exclusively, I have all the proof I need every day in my practice to justify these modalities.”11
Another key source of the incompatibility of CAVM and EBM is the problem of vitalism. At the heart of most alternative approaches, whether explicit or hidden, is a belief that living entities are defined by nonphysical energetic or spiritual forces, and health cannot be maintained or restored by any system that does not account for these forces. Homeopathy, chiropractic, Reiki and other “energy” therapies, traditional Chinese medicine (from which derive most of the forms of acupuncture practiced today), and many other CAVM approaches were born from this pre-scientific belief in spiritual forces as the cause of disease.
While proponents of many of these methods have tried to paint over this idea with more modern scientific language (referencing quantum physics or bioelectricity, for example), the concepts often remain central to their practices.
“Acupuncture reconnects and balances Life energy.… Energy medicines such as homeopathy, homotoxicology, Reiki, craniosacral therapy, and others align the physical, mental, and spiritual portions of the organism. Yes, I did say spiritual and that is a big part of holistic medicine—recognizing the spiritual nature of Life.”12
“pharmacological and surgical approaches appear incomplete…because they ignore the Vital Force which animates and breathes life into the biomachinery of living systems”13
“Because medical science has defined itself on a strictly physical basis, it is true that vitalism is unscientific. By definition, vitalism embraces a concept about a nonphysical force that can never be understood within the current scientific, medical paradigm.”14
“The belief that spiritual, emotional, psychological, or other non-measurable aspects of the individual patient’s presentation are important for healing does not require one to reject evidence obtained from clinical trials, but it does require the recognition that knowledge gained from such methods will be insufficient to guide optimal clinical practice…The importance of Qi in traditional Chinese medicine means that research that cannot and does not account for the force will never be compelling for a practitioner.”15
Even when disavowed, these mysterious forces leave gaps in causal reasoning left unfilled by scientifically legitimate concepts. Chiropractors have largely replace Palmer’s “innate intelligence” with the “vertebral subluxation complex,” but this has not been convincingly shown to exist.16 The “energy” behind Reiki and other supposed energy therapies cannot be detected except by those who already believe in it.17 And for all the thousands of pages devoted to finding a consistent, predictable reason why acupuncture should have beneficial clinical effects, no clear and compelling mechanism has been demonstrated.16 All of these methods, and even some more plausible CAVM practices such as herbal medicine and laser therapy, use scientific language to cover the core principle, which is some undetectable magical force inconsistent with a scientific understanding of physics and biology.
The Conflict: Practice The most unfortunate aspect of CAVM is that it is largely defined and marketed in opposition to science-based medicine. Using it requires at least some level of acceptance of principles and forms of evidence not compatible with an evidence-based approach; and all too often it requires an outright rejection of mainstream medicine.
Use of alternative therapies is associated with less confidence in science-based medicine and less effective use of conventional tests and treatments.18–20 This, in turn, is associated with poorer outcomes, such as shorter survival in cancer patients and greater risk of preventable infectious disease with vaccine refusal. While there is scant evidence to support claims that integrating alternative therapies with scientific medicine improves outcomes, it is clear that it can sometimes worsen them.
Both the growing popularity of alternative treatments and the growing suspicion of science and science-based medicine stem from the same cultural and political factors, issues that have little to do with what is actually best for patients.
Ideally, every idea for assessment and treatment of our patients would go through the necessary steps of scientific evaluation:
development of a biologically plausible theoretical foundation compatible with established knowledge
validation of this foundation and demonstration of possible benefits and risks in pre-clinical research
testing in real-world patients through properly designed, conducted, reported, and replicated clinical trials
Not every step is always possible, and the evidence we have is often flawed and incomplete, for both science-based and alternative medicine. But this path is at least the aspiration of EBM, while is generally not seen as necessary or even desirable for CAVM. While EBM looks forward, developing new interventions and abandoning those that deserve to be left behind, CAVM looks backwards, mining the pre-scientific past for ideas and then setting out to create the impression of modern, scientific legitimacy without a genuine willingness to reject them if the data says we should.
Individual therapies may begin in the CAVM domain and pass into truly evidence-based practice. And some apparently science-based practices may drift into CAVM if evidence develops suggesting they should be abandoned but practitioners are unwilling to do so. However, for the most part CAVM and EBM will remain incompatible, oil and water, interacting but separated by incompatible philosophies, epistemologies, culture and politics, and fundamentally different views of how we should judge our practices.
References
1. College of Integrative Veterinary Therapies. College of Integrative Veterinary Therapies. Accessed October 14, 2025. https://civtedu.org
2. Marsden S. The New Era of Evidence-Based Medicine: Can We Survive It? American College of Veterinary Botanical Medicine Blog. May 11, 2025. Accessed October 14, 2025. https://acvbm.blog/2025/05/11/the-new-era-of-evidence-based-medicine-can-we-survive-it/
3. Barbieri CR. Impact of Distant Reiki on Owner Assessment of Health and Wellbeing of Adult Dogs: A Blinded, Placebo-controlled, Randomized Trial. J Am Holist Vet Med Assoc. 78(Summer):11-19.
4. Traditional, Complementary and Integrative Medicine. Accessed October 14, 2025. https://www.who.int/health-topics/traditional-complementary-and-integrative-medicine
5. Angell M, Kassirer JP. Alternative medicine–the risks of untested and unregulated remedies. N Engl J Med. 1998;339(12):839-841. doi:10.1056/NEJM199809173391210
6. Churchill W. Implications of evidence-based medicine for complementary and alternative medicine. J Chin Med. 1999;59:32-35.
7. Barry CA. The role of evidence in alternative medicine: contrasting biomedical and anthropological approaches. Soc Sci Med 1982. 2006;62(11):2646-2657. doi:10.1016/j.socscimed.2005.11.025
8. Minchin T. Storm. Orion Publishing; 2014.
9. Jagtenberg T, Evans S, Grant A, Howden I, Lewis M, Singer J. Evidence-based medicine and naturopathy. J Altern Complement Med N Y N. 2006;12(3):323-328. doi:10.1089/acm.2006.12.323
10. Curtis P. Evidence-Based Medicine & Complementary & Alternative Therapies. In: Curtis P, Gaylord S, Norton S, eds. The Convergence of Complementary, Alternative, and Conventional Health Care: Educational Resources for Health Professionals. UNC School of Medicine, Program on Integrative Medicine; 2004:Chapel Hill, NC. Accessed October 16, 2025. https://www.med.unc.edu/phyrehab/pim/wp-content/uploads/sites/615/2018/03/Evidence-Based-Med.pdf
11. Jewell G. Comments on practising complementary and alternative modalities. Can Vet J. 2000;41(5):351.
12. Kerns N. Alternative views on canine holistic dog care. Whole Dogs Journal. September 13, 2007. Accessed October 16, 2025. https://www.whole-dog-journal.com/care/alternative-views-on-holistic-dog-care/
13. Stefanatos J. Introduction to bioenergetic medicine. In: Schoen A, Wynn S, eds. Complementary and Alternative Veterinary Medicine: Principles and Practice. Mosby; 1998:227-245.
14. Knueven D. An introduction to holistic medicine. In: The Holistic Health Guide: Natural Care for the Whole Dog.TFH Publications; 2008:9-13.
15. Tonelli MR, Callahan TC. Why alternative medicine cannot be evidence-based. Acad Med J Assoc Am Med Coll. 2001;76(12):1213-1220. doi:10.1097/00001888-200112000-00011
16. McKenzie BA. Placebos for Pets?: The Truth About Alternative Medicine in Animals. Ockham Publishing; 2019.
17. Rosa L, Rosa E, Sarner L, Barrett S. A Close Look at Therapeutic Touch. JAMA. 1998;279(13):1005-1010. doi:10.1001/jama.279.13.1005
18. Johnson SB, Park HS, Gross CP, Yu JB. Complementary Medicine, Refusal of Conventional Cancer Therapy, and Survival Among Patients With Curable Cancers. JAMA Oncol. 2018;4(10). doi:10.1001/jamaoncol.2018.2487
19. Cordonier L, Cafiero F. ?The link between interest in alternative medicine and vaccination coverage?. Rev Eur Sci Soc. 2023;611(1):175-197.
20. Cramer H, Bilc M. Use of complementary medicine and uptake of COVID-19 vaccination among US adults. Front Med. 2025;12:1474914. doi:10.3389/fmed.2025.1474914
I am preparing a series of lectures for an upcoming conference, and it has given me a chance to reflect on some of the core ideas that have always driven this blog– the challenges created by our human limitations and the strategies we have develop to mitigate them.
This lecture attempts to illustrate what evidence-based medicine is and, perhaps more importantly, why we need it. In this current Age of Endarkenment, when science is under attack and misinformation is rampant, such reflection is more important than ever.
Our Shared Malady Evidence-based medicine (EBM) is a treatment for a disease most of us don’t realize we have. It is both a preventative and a treatment, really, but it is not a cure. The best we can hope for is to manage the symptoms and minimize the damage done by our disease.
The disease we suffer from lies in our brains. The mechanisms of observation and judgement we rely on as veterinarians to make recommendations for our patients are riddled with lesions. These have names like confirmation bias, cognitive dissonance, logical fallacy, and many others. The forms and manifestations of our disease are legion.1,2
The consequences of our illness are, sadly, experienced mostly by our patients. Misdiagnosis, overdiagnosis, rejection of effective therapies and use of ineffective ones, and ultimately suffering and death that could, perhaps, be avoided if we sought treatment for our condition.
Like many medicines, EBM, can be bitter and uncomfortable to take. Many of us don’t know we need it, and even when we are diagnosed we may reject the treatment as too unpleasant. And there are potential adverse effects from treatment. A clear understanding of our limitations can be overwhelming, leading to despair and even therapeutic nihilism. However, the potential benefits are great and worth the risks.
Before I describe the treatment, I need to characterize the disease and convince you that you have it. This is especially difficult because the features of our malady include elements specifically inhibiting our ability to recognize it. Confirmation bias blinds us to evidence of our illness. Cognitive dissonance causes pain when we are forced to see and acknowledge such evidence. The Dunning-Kruger effect makes those of us least knowledgeable about the illness feel the most confidence that we are free of it.
The best way to start on our journey may be with a story. Once there was a doctor, a kindly man who cared for children named Dr. Spock. He was an intelligent, caring doctor who brought great progress to the field of pediatrics and parenting. He wrote a book for parents called The Common Sense Book of Baby and Child Care,3 that sold millions of copies, was translated into 29 languages, and became a worldwide guide for parenting.
One key piece of advice Dr. Spock gave parents was that they should always put their babies to sleep on their stomach. Decades of experience, and simple common sense, showed Dr. Spock that doing so would reduce the risk of aspiration if an infant vomited, and this would help prevent Sudden Infant Death Syndrome (SIDS). SIDS is a terrifying and poorly understood condition in which apparently healthy babies die without warning, and parents are desperate for any action they can take to prevent it.
From the publication of Dr. Spock’s in 1946 until the early 1970s, the practice of putting infants to sleep on their stomachs was widely adopted, and parents were reassured by the confident recommendation of their doctors to follow this practice.
However, by the 1970s, abundant research had accumulated showing this practice was a mistake. Babies sleeping on their backs were actually more likely to die of SIDS.4 Despite this evidence, the practice persisted until the early 1990s. For twenty years, parents around the world did the wrong thing, even after science had showed it was wrong, because of cultural inertia, confidence in respected authorities, anecdotal experience, and all the other sources of our confidence in mistaken beliefs.
A review published in 2005 found that heeding the evidence and abandoning the traditional practice sooner might have saved the lives of 10,000 children in the U.K. and 50,000 in Europe, the U.S., and Australasia.4 When educational efforts finally reached parents, and they began putting babies to sleep on their backs, the rate of SIDS dropped markedly.
Figure 1. SIDS rate versus prone sleeping rate in the United States, 1983 to 1995 (from Carroll, 19985)
Does this mean Dr. Spock was a bad doctor? A fool? Were parents around the world stupid? No! This tragedy was a consequence of the illness we all suffer from- a natural tendency to see our personal observations and the stories told by others as compelling and reliable guides to reality, and a lack of a deep, effective appreciation of our limitations and the advantages of scientific data over anecdote and plausible reasoning.
Evidence-based medicine is “the conscientious, explicit, and judicious integration” of controlled research evidence with our clinical expertise and judgement and the goals and values of our clients.6,7 It is not a rejection of the value of the observations and judgements we make, but a recognition of their limitations and the dangers of trusting them too far. It is a set of methods and practices, yes, but first and foremost it is a philosophy, a perspective. “At its heart is the confidence in the scientific methodology that has developed over the centuries to enable us to distinguish what is likely to be true from what is likely to be false.”8 Diagnosing the illness, admitting we have a problem, is the necessary first step for starting treatment. I can teach you a bit about the treatment and how it works, but it won’t help you if you don’t begin by seeing that you need treatment.
Does EBM Work? Proving that EBM is effective is not a simple matter. Where is the completely omniscient and objective observer who can judge that one approach to knowledge is better than another? Who would be willing to admit to practicing opinion-based medicine or belief-based medicine and then be willing to participate in a scientific study to show that their approach is better (or worse) than science?
The best we can do is make some logical inferences, though I personally think these are quite compelling. Consider the change in human life expectancy over time (Fig. 2)
Figure 2. Life expectancy around the world
While this chart starts in the 18th century, the available evidence suggests that the flat line, with overall life expectancy less than 40 years, could be extended many thousands of years into the past. Figure 3 shows a major reason for this, which is the high proportion of human children who did not survive to adulthood for most of human history.
Figure 3. Childhood mortality.
For the vast majority of human history, most humans didn’t survive childhood (or childbirth), and we were plagued with parasites and infectious diseases, malnutrition, and a host of other acute and chronic ills. While a lucky few in each generation managed to live to old age, the great majority could expect only the Hobbesian reality of a “poor, nasty, brutish, and short” life. And then, in a mere handful of centuries, that changed.
Today, we enjoy a length of life and a state of health and wellbeing unimaginable to even the most fortunate of our ancestors. What changed? Did we evolve physically? Did the environment become more hospitable? The gods kinder?
The answer is simple and profound- science. All that changed was our ability to understand nature. Over centuries, we developed the methods of scientific thought and practice that led to a more accurate understanding of the causes of illness and death. And with that improved understanding came both new techniques for treatment and prevention, and also new methods for testing those techniques.
We are using the same brains our ancestors used. In our daily life, including in clinical practice, we still observe and reason as they did, and we make all the same errors. But we defer often enough to the picture of reality built by the community of scientists using scientific methods that we end with better information and making better choices.
EBM is just an extension of this set of methods. The basic steps, and all the detail and nuance embedded in them, are all simply a practical application of the principles and methods of science to clinical practice. Deciding, then, whether EBM is worth using depends largely on deciding whether science is better than the alternatives that preceded it. The alternatives most propose—relying more on clinical experience, tradition, or reasoning from theoretical principles- are the same that guided medicine in all the centuries before the changes in figures 2 and 3 began.
The Basics of EBM The core of EBM in practice is quite simple. It consists of five basic steps-
Ask a question
Locate relevant evidence
Evaluate this evidence
Draw a conclusion
Assign a level of confidence
These steps are repeated as often as necessary until we feel we know enough to take action. They are repeated again whenever we have new questions, new evidence appears, or new action is needed. Entire textbooks have been written to guide us through these steps, but the basic process comes down to this.
The Question The first step is to identify what we need to know to care for a given patient. What tests should we run? What treatment should we use? How can we tell if the treatment is working? What can we tell the owner about risks or prognosis?
The key to getting useful answers from the scientific literature is asking useful questions. They should be specific enough to turn up relevant evidence but not so narrow that we exclude useful information. “Do antibiotics work?” is too broad to be meaningful. “Should we use amoxicillin, cephalexin, or enrofloxacin, for one week or for two weeks, in a 9 year-old neutered male Labrador retriever with an infected laceration from a stick on the front limb?” is not going to turn up many relevant clinical studies. Learning how to organize or ignorance and structure our questions is an EBM skill that can be developed, and there are many resources to support this.
Finding the Evidence Another critical EBM skill is learning how to locate useful evidence. Sources as varied as textbooks, scientific journals, online databases and discussion forums, and even the vet working in the office next door are all available, and they all have their strengths and weaknesses. The best evidence is often the scarcest and hardest to access, while the most convenient sources often come with the greatest limitations. Locating and acquiring evidence requires us to be a bit like a detective or someone on a scavenger hunt, which can be fun but can also take time we don’t have. Building a collection of skills and resources over time can reduce the burden of finding useful evidence.
Evaluating the Evidence It would be ideal if we could simply read a published scientific study or listen to the advice of our colleagues and immediately put the information we find into practice. Unfortunately, not all evidence is equally reliable, and even high-quality data may not apply to the patient in front of us. Critical appraisal of evidence is arguably the most important, and the least used step in this list.
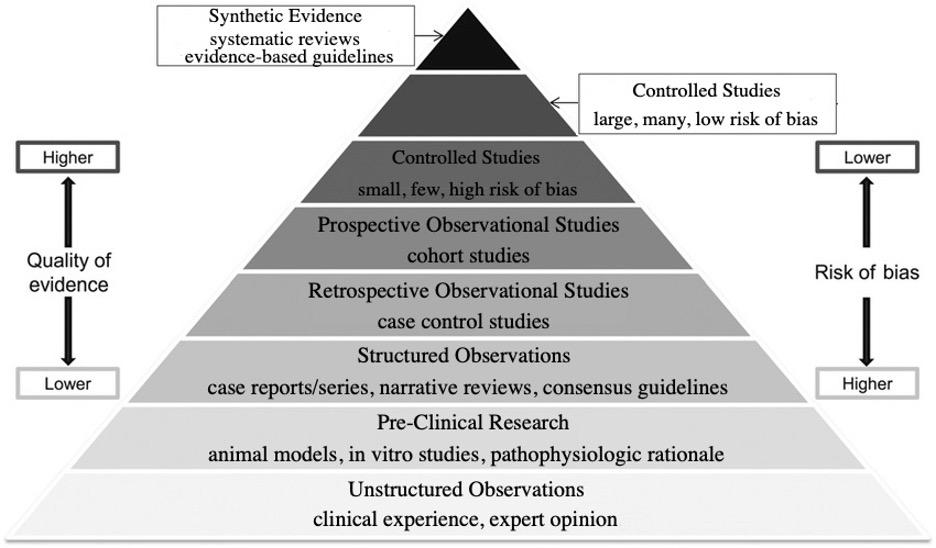
There are shortcuts that can help us. The classic pyramid of evidence in Figure 4 illustrates an approach to evidence that is sophisticated but academic and not always useful in practice.
Figure 4. Traditional evidence pyramid.
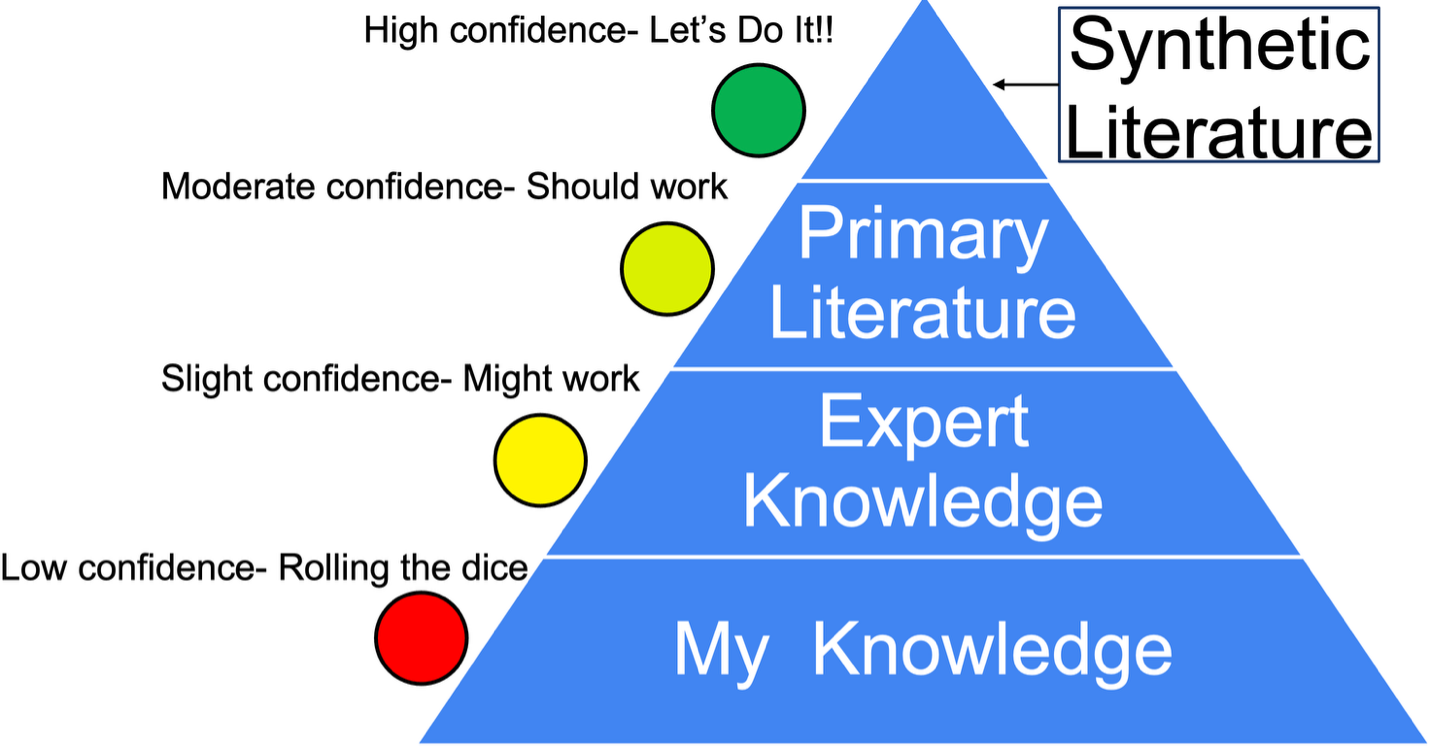
I prefer a simpler scheme which is more easily applied for most of us.
Figure 5. Practical evidence pyramid.
This emphasizes that all sources of evidence are potentially useful, but the closer we get to the top of the pyramid, the more confidence we can have in the information. Synthetic resources, such as clinical practice guidelines and systematic reviews, are especially valuable since they are both high in reliability and efficient, requiring less time, effort, and expertise to use effectively.
The Conclusion and the Confidence Once we have gathered the available evidence and evaluated it, our main job is to decide what it means. What actions should we take or avoid based on the evidence? Just as important as the conclusion we reach is the level of confidence we assign to it. If I choose to say, “Here is a powerful therapy which will cure your cat,” that sets up very different expectations and behavior, in the owner and in myself, than if I say, “Here’s a therapy a few people have tried in dogs that might help your cat.” For reasons both practical and ethical, it is crucial that we choose and communicate an appropriate level of confidence for the recommendations we make.
Our disease drives us to have confidence greater than warranted by most of the evidence we are likely to have available. EBM gives us both a warning and some techniques for setting a more appropriate level, which then encourages more truly informed consent from our clients and probably more reasonable expectations and better followup.
The Madness and Wisdom of Crowds Let us end with another story. On a cold Thursday morning in December, 1799, the former president of the United States, George Washington, rode out into the snow to inspect his farmlands.9 He was 68 years old, but strong and healthy for his age. That night he developed a bit of a sore throat, and by a day later he was having a hard time breathing.
Unable to swallow a remedy of vinegar, molasses, and butter due to swelling in his throat, he accepted his doctor’s suggestion to remove a half pint (about 240mls) of blood from his arm. The patient did not improve, and the procedure was repeated several times over the day, with various doctors removing a total of about 3 to 4L of blood (about a third to half of the typical total blood volume for an adult man). Despite these heroic efforts, the former president died after about 13 hours of intensive treatment.
Bloodletting has been a routine and respected therapy in many cultures around the world and in many different historical eras. It is based on a simple powerful idea: What if we all illness stemmed from a derangement of a few essential factors, and we could prevent or cure illness simply by keeping these in balance?
This idea is intuitively appealing, clear, and logical. It is also, of course, wrong. But every time it has emerged, it has captured the imagination and deep faith of the brightest medical and scientific minds, and persisted for centuries, even millennia, and into the present day.
A reasonable catchall name for this view is humorism. It was the rationale for the treatment of bloodletting promoted by Hippocrates in the 5th century BCE and accepted by George Washington’s doctors in 1799. Some versions of humorism persist today in the theories of Traditional Chinese Medicine and Indian Ayurveda.
There have always been skeptics of bloodletting. George Washington’s wife opposed the practice and begged his doctors not to take so much blood from her husband. But the logic of humorism and the innumerable anecdotes of patients cured by the practice overcame such skepticism. As late as 1875, defenders of the practice argued for it with reference to such compelling evidence:
“Who is there with ten or twenty years experience in the profession, that has not seen the most marked advantages from bleeding…” asked one such defender.10 Another learned physician wrote that, “He thought it really saying too much…that we should assume to be so much wiser than our fathers, who had lent their approval to a custom that had been sanctioned by ages of experience.”10
Eventually, the current models of physiology and disease replaced humorism, and the methods of science replaced bloodletting with a range of practices that, while imperfect, have nearly doubled human life expectancy and brought levels of health and comfort unimaginable in most of human history.
So were all our “fathers” bad doctors? Fools? No! This story is meant to show the unique and challenging nature of our disease. It is both congenital, built into each of our brains from birth, and also communicable. The manifestations of this illness in each of us magnifies the symptoms in others, and in a population the disease can make us sicker and do more harm that in one isolated patient. We can reinforce and sustain each other’s beliefs, even if they are egregiously wrong.
Fortunately, the same power of the community lies in the treatment for our illness. Science is a community process in which we pit our limited, imperfect, biased notions against each other in a competition judged by the strength and consistency of the data we can produce. Though the madness of crowds11 can lead us horribly astray, the wisdom of crowds12 can rescue us from our individual delusions. The secret is to harness the competition of ideas in a race governed by the rules and standards of science and evidence.
Evidence-based medicine is a part of the larger project of using science to control our illness, to keep us closer to the truth of nature so we can help our patients most effectively.
Key Points
Human observation and judgement is inherently flawed, and our confidence in our reasoning is typically greater than the true accuracy of our beliefs.
Evidence-based medicine (EBM) is a facet of the greater project of science. It is a set of perspectives and practices meant to improve the accuracy of our understanding of nature and set appropriate degrees of confidence around our beliefs.
The five basic steps of the EBM method are-
Ask a question
Locate relevant evidence
Evaluate this evidence
Draw a conclusion
Assign a level of confidence
This is an iterative process, repeated often as our information needs and the available evidence change.
Groups of humans can strengthen and persist in false beliefs for generations.
Groups of humans can also develop more accurate understanding of nature if guided by the methods of science
Individual clinicians can benefit from EBM by
Maintaining an awareness of our disease and its consequences
Following the steps of EBM
Relying on the work of a scientific community more than on individual personal experience and belief
References 1. Kida T. Don’t Believe Everything You Think. Prometheus; 2006. Accessed October 9, 2025. https://www.simonandschuster.com/books/Dont-Believe-Everything-You-Think/Thomas-E-Kida/9781591024088
2. McKenzie BA. Veterinary clinical decision-making: cognitive biases, external constraints, and strategies for improvement. J Am Vet Med Assoc. 2014;244(3):271-276. doi:10.2460/javma.244.3.271
3. Spock B. The Common Sense Bookf of Baby and Child Care. 1st ed. Duell, Sloan, ad Pearce; 1946.
4. Gilbert R, Salanti G, Harden M, See S. Infant sleeping position and the sudden infant death syndrome: systematic review of observational studies and historical review of recommendations from 1940 to 2002. Int J Epidemiol. 2005;34(4):874-887. doi:10.1093/ije/dyi088
5. Carroll JL, Siska ES. SIDS: counseling parents to reduce the risk. Am Fam Physician. 1998;57(7):1566-1572.
6. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312(7023):71-72. doi:10.1136/bmj.312.7023.71
7. Straus SE, Glasziou P, Richardson WS, Haynes RB. Evidence-Based Medicine: How to Practice and Teach EBM. 5th ed. Elsevier; 2019.
9. Vadakan V. The Asphyxiating and Exsanguinating Death of President George Washington. In: 2004. Accessed October 9, 2025. https://www.semanticscholar.org/paper/The-Asphyxiating-and-Exsanguinating-Death-of-George-Vadakan/33f243e97580948b73e700df9489906a37849247
10. McKenzie BA. Placebos for Pets?: The Truth About Alternative Medicine in Animals. Ockham Publishing; 2019.
11. Mackay C. Extraordinary Popular Delusions and the Madness of Crowds. chard Bentley; 1841.
12. Surowiecki J. The Wisdom of Crowds. First Anchor books edition. Anchor Books, a division of Random House, Inc; 2005. Accessed October 9, 2025. http://catdir.loc.gov/catdir/samples/random051/2003070095.html
I was recently privileged to give a brief talk at the Hill’s Global Symposium focusing on aging in veterinary patients. This is a very quick summary of merely one example of how understanding aging mechanisms can create opportunities for developing treatment to give our patients longer, healthier lives.
This article does a good job of articulating the issue with only a bit of the unfortunate false balance so common in media coverage of anti-vaccine activism, alternative medicine, and other extreme viewpoints.
The newspaper also provided a brief guide to vaccination for pet owners which is less detailed than veterinary guidelines (e.g. those from the American Animal Hospital Association for dogs and cats) but which does address some important questions.