
This an article I wrote for Veterinary Practice News about our hospital experience with the COVID-19 pandemic. Every veterinary clinic and hospital will have their own unique experience of this time, but I suspect much of this will look familiar to others in the profession and to pet owners. One element of the experience that is relevant to my work here on SkeptVet is the importance of a critical, flexible, evidence-based approach, which has helped us tremendously in dealing with the unprecedented challenge.
From the trenches: How life has changed since COVID-19 came into our lives: What veterinary medicine is like at Californina’s ground zero
The hospital is quiet as I walk in at the start of my shift. The usual bustle of clients, staff, and animals has been replaced by empty hallways and only a few masked doctors and nurses going about their work quietly, careful to keep their distance from each other. I stop at the screening table and start my day by taking my temperature. It is under 100.4 F, and I have no cough or other respiratory symptoms, which means I can work today.
I set down my belongings at my desk and go to change my clothes. I wear scrubs every day now, and I have a pair of dedicated work shoes that stay at the hospital. I also have a collection of beautiful cloth face masks sewn by one of our employees—I wear a clean one every day.
At the end of my shift, all of my work clothes go into the laundry. When I get home, everything I took to work stays in the garage. I pass quickly through the house and take a shower before I greet my family. I am especially mindful to keep my distance from my elderly mother, who lives with us, and to handle neither her dishes nor her medications. My wife does that now, since she has been working from home and hasn’t mingled with people outside the house for the last month. This is the new routine of our lives, one familiar to countless others since the arrival of COVID-19.
Operating in California’s ground zero
I have worked at the same practice for 16 years. We are an unusual hospital; an independent general practice with 30 veterinarians and more than 150 other staff, open 24 hours a day seven days a week. Because we are located in Silicon Valley, an affluent area in Santa Clara County, Calif., we able to offer services not always found in first-opinion practices, such as orthopedic surgery, in-house ultrasound, cancer therapy, and advanced emergency and intensive care. Our location, however, also means we are in the center of California’s novel coronavirus outbreak. COVID-19 has changed not only my morning routine, but nearly every aspect of the work and lives of our practice, staff, and clients.
Santa Clara identified the first case of COVID-19 in the county (and the ninth in the U.S.) in early February. A sentinel surveillance study in early March confirmed community spread was already occurring, and the county began instituting social distancing measures on March 11. Initially, these involved closure of some public businesses and recommendations for people to avoid large gatherings. By March 16, Santa Clara and surrounding counties had issued shelter-in-place orders, essentially banning people from leaving home except for specified essential activities. On March 30, further restrictions were added and the shelter order was extended into May.
This rapidly expanding public health crisis and frequent changes in restrictions on public activity has presented a tremendous challenge to our hospital. We see hundreds of patients and have dozens of doctors and nurses in the building every day. We also operate on an open hospital model, meaning clients can stay with their pets for nearly every aspect of their care, from being present for outpatient procedures, to watching surgeries, to sitting with hospitalized patients as long as they choose during daytime hours. While this model is unfamiliar and startling to many in the veterinary profession, it has been an intrinsic component to our practice culture for decades. Having clients present throughout the hospital is something we, and our clients, have come to expect.
Doing things differently
The coronavirus outbreak and the public health directives aimed at combating it have forced us to reevaluate our models for patient care, client service, and personnel management; our financial structures and processes; and even our role in the larger public health landscape. Such a comprehensive reevaluation of every aspect of our work, conducted rapidly and in an ever-changing environment, has been challenging, even painful. However, it is also an opportunity to take stock of who we are as health-care providers and as a business, and to grow stronger as a result.
In addition to seeing patients, part of my job in my practice is to drive and support continuing improvement in the quality of care we provide, and to help maintain staff and patient safety. I am the designated evidence-based medicine nag, responsible for translating scientific research into useful tools and actions we can take to better care for our patients. This includes training new veterinarians; developing protocols and guidance documents; conducting clinical audits and evaluating patient outcomes; and many other quality-improvement activities.
One particular project that has proven timely was my effort last August to promote more effective hand hygiene throughout the hospital. I expanded the accessibility of hand sanitizer, put up posters throughout the hospital illustrating proper handwashing technique, and of course nagged everyone to wash their hands. Lately, some staff members have jokingly suggested I may have gone a bit overboard in trying to make my point.
Of course, despite my efforts to support a culture of proactive, science-based medicine, we could not realistically have been fully prepared for what the coronavirus pandemic has required of our practice. However, this culture has proven useful in making the many adjustments necessitated by the virus in the face of limited evidence and great uncertainty. We already had a system for identifying reliable sources of information and translating imperfect science into clinical practices. Our doctors, staff, and management were long accustomed to incorporating scientific data into their daily activities and to adjusting their work routines based on changes in the available evidence. The habits of flexible, pragmatic evidence-based medicine have served us well.
The specific changes we have made in how we handle clients and patients, how we protect staff, and how we have adjusted our business to cope with the legal and economic realities of the pandemic may or may not be useful to other practices in other contexts. However, they illustrate how the methods and habits of evidence-based medicine can help a veterinary practice respond to an unexpected and unfamiliar crisis.

Applying evidence-based medicine
We began our response to the pandemic by developing and collecting policy documents in one central location. With a rapidly changing environment, and frequent adjustments to policies and procedures, it was crucial the most current protocols be readily available to everyone on staff. Protocols were developed by a group representing all the teams within the practice, including doctors, technicians, and management. Input was sought from as many people as practicable, which frequently helped to identify oversights and errors, as well as to generate the widest possible array of ideas and options.
Although veterinary practices are considered essential services in our region, and therefore allowed to operate despite the restrictions of public health orders, we realized early we would need to limit our work to urgent and emergent cases, and to defer most elective and well-pet services to reduce traffic through the hospital and exposure risk to staff and clients. We developed a triage tool to help staff decide which services qualified as essential and which would need to be deferred. This was similar to the tools developed by the British Small Animal Veterinary Association (BSAVA) and other veterinary organizations.
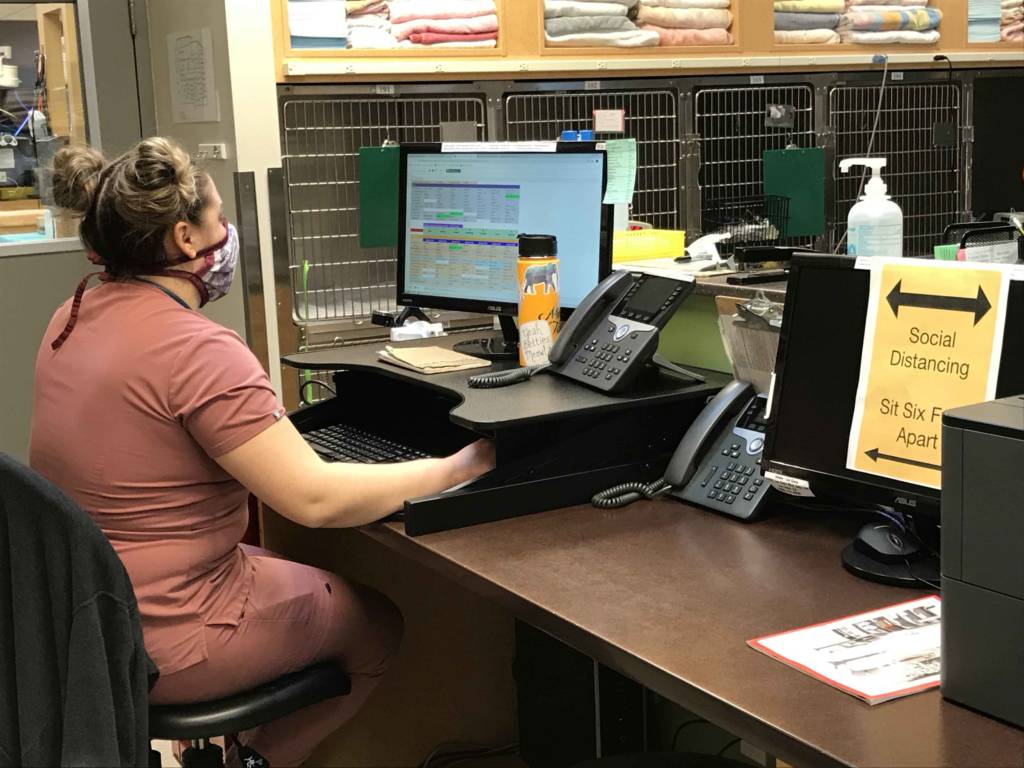
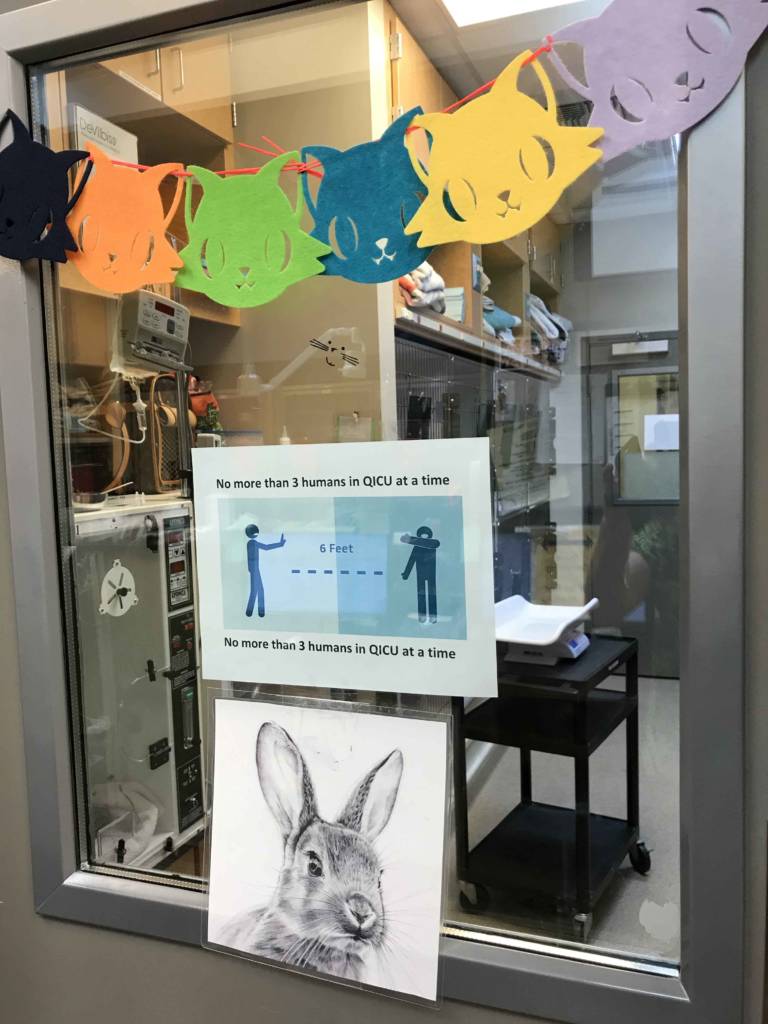
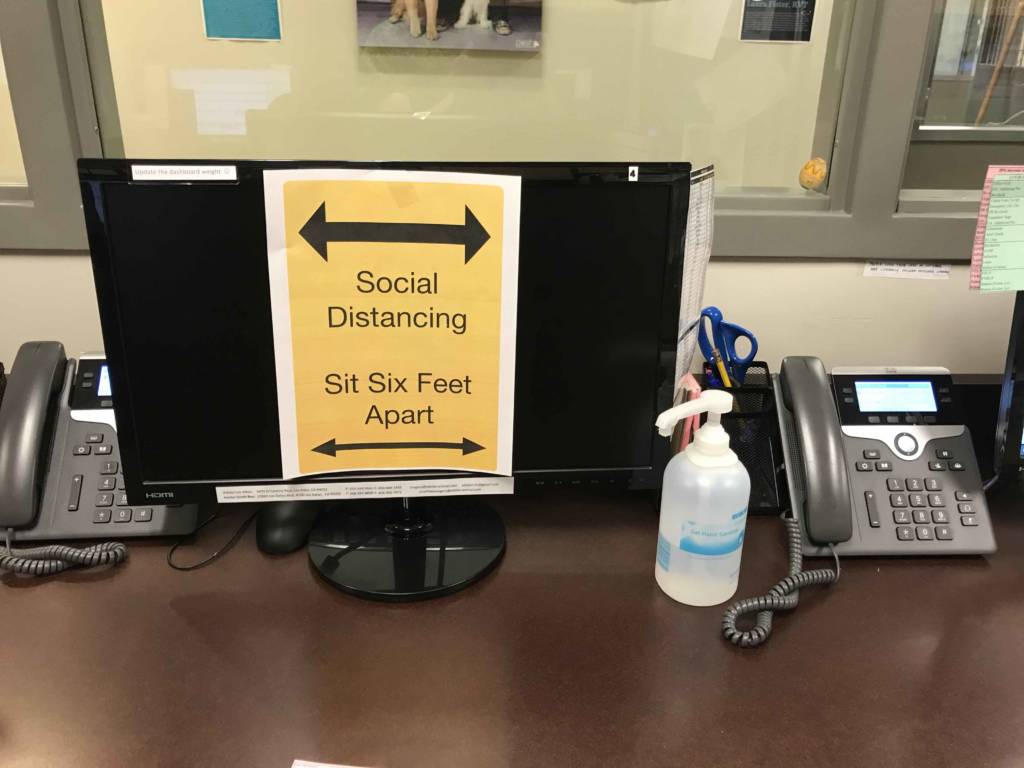
Our initial strategy for reducing exposure risk was to screen both staff and clients for relevant clinical symptoms and for fever. Though this strategy is imperfect, it has been utilized and found helpful for identifying COVID-19 cases in some circumstances. We also set up social distancing guidelines within the hospital.
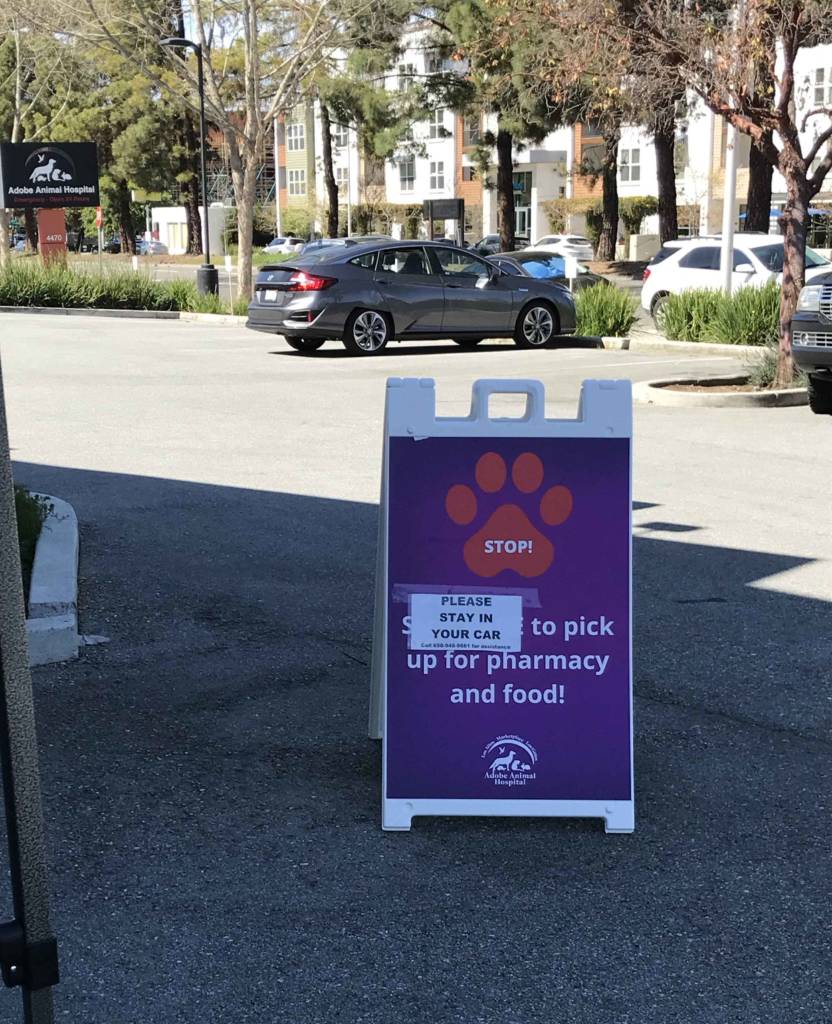
However, we quickly realized these measures were insufficient, and we made the difficult decision to ban all clients from the hospital, apart from exceptional circumstances such as euthanasia and critical acute emergencies. Clients now wait in their cars, and nurses in appropriate personal protective equipment (PPE) triage pets outside and then bring them into the hospital. All subsequent communication with clients is by telephone until the pet is returned to them outside.
This has been especially difficult for us, and for our clients, as it conflicts with our culture as an open hospital. Being separated from a sick pet is an unfamiliar experience and an added stress for clients who, like all of us, are already dealing with the impact of the pandemic in their personal lives. Most clients have been understanding of our goals in protecting them and our staff, but in the short-term, this has been one of the most uncomfortable consequences of the outbreak. The long-term effects on our culture and relationships with the community are a source of concern for all of us.
Watching out for one another
Having restricted client access to the facility, the greatest risk to our own health became each other. It is often impractical to maintain effective physical distancing when working together treating patients. In response to this risk, we have continued screening staff for symptoms and fever, and we have done what we can to keep people apart in the workplace. The extra hand sanitizer I ordered in September and the handwashing protocols I posted have turned out to be quite useful! We have also had many lively discussions about the use of masks as a tool for reducing the risk of coronavirus transmission within the hospital.
The evidence concerning the value of masks in reducing spread of respiratory viruses is limited and contradictory (e.g. 1, 2, 3). It seems unlikely they protect the wearer from exposure, and they can actually increase risk if improperly used. However, wearing masks may reduce the risk of an infected person from spreading the virus, particularly since asymptomatic shedding apparently occurs commonly. It is also important to remember PPE is in short supply, and the risk and needs faced by human health-care providers are much greater than ours.
Early in the outbreak, our hospital donated a substantial portion of our masks, gowns, and gloves to a local hospital, as well as offered our ventilator for use in human patients through a database set up by the American College of Veterinary Emergency and Critical Care (ACVECC). Our remaining PPE is under lock-and-key, to be used only when strictly necessary.

Ultimately, the mask debate was settled for us by a directive from public health officials recommending the use of cloth masks in addition to physical distancing methods in businesses still operating. We are fortunate to have several employees with handicraft skills who have been making beautiful and functional cloth masks for our staff and their families. These employees have had plenty of time for such projects, as another necessary response to the pandemic has been to reduce staff in the hospital and to decrease payroll expenses.
The limitation of cases to urgent and emergent care has dramatically reduced revenue at our hospital. Veterinary small animal medicine is an unusual hybrid, being both a health-care industry and also, in many cases, a small business enterprise. Large-scale corporate ownership and consolidation of veterinary practices is certainly widespread and growing. However, the average small animal practice in the U.S. employs only two veterinarians and three to five veterinary technicians (2019 AVMA economic report). Though my practice is unusually large, we are still a much smaller business than most human health-care providers.
The drop in revenue, as well as the need to reduce the risk of coronavirus spread between employees, has necessitated dramatic cutbacks in staffing at our hospital. These reductions have involved unpaid leave, furlough, and various mechanisms dictated by the financial and regulatory environment in which we operate. Most doctors, myself included, now work one week and are furloughed for one week. Other staff members are limited in the number of shifts they can work in a month. So far, we have managed to avoid laying off any employees, but the threat to our livelihood adds to the stress imposed by the risk to our health.

Overcoming disruption
As in veterinary practices around the world, our employees are struggling to face not only restrictions on their movement and activities, cancellation of planned events, closure of schools and loss of childcare, and other disruptions in their personal lives, but also a loss of income and of the security and purpose of their jobs, which for many are as much a vocation as an occupation.
Like many in the developed world facing isolation and uncertainty due to the pandemic, the role of virtual communication in our lives and businesses has expanded greatly. We have a dedicated private Facebook community for staff that has provided great support for many of us during the days we cannot work. We are, in some ways, closer than ever since we are learning more about each other’s homes and hobbies, partners and pets through this virtual community.
We are also making use of online communication tools as a hospital. In April 2019, we began offering video visits for clients. These have been a useful way of triaging patients and managing minor health problems that do not necessarily require an office visit. As a result, we had a reliable system and experienced telemedicine staff in place when the pandemic began. Since the outbreak began, the U.S. Food and Drug Administration (FDA) has relaxed requirements for a veterinarian-client-patient relationship to facilitate such use of telemedicine tools. We now have two full-time telemedicine doctors, and this has proven an excellent means of maintaining contact with clients and preserving revenue, while reducing hospital visits and exposure risk to employees and pet owners.
Since the beginning of the pandemic, our clients and staff have had questions about the risk of infection to our patients and the potential for pets to spread the virus to humans. Despite the enormous, unprecedented scientific research effort targeting COVID-19, there is surprisingly little evidence to help answer these questions.
Very few studies have specifically evaluated the susceptibility of companion animals to SARS-CoV-2 or the risk for transmission from dogs and cats to their owners or veterinary personnel. Individual case reports and limited research evidence suggest dogs are very resistant to infection and illness (4, 5, 6). Cats and ferrets appear to be more susceptible, but the risk of transmission to humans is still considered low (6, 7, 8, 9). There is essentially no research evaluating the potential for pets to act as fomites or mechanical vectors for COVID-19 (10).
We have developed guidelines in our hospital for handling pets from known COVID-19-positive households, both those with or without symptoms, and there are a number of such guidelines available from veterinary organizations (11). However, all of these are based on extremely limited evidence, and it will be some time before we fully understand what risk, if any, pets may pose to veterinary professionals or the public. This is an example of the common, but necessary challenge of practicing evidence-based medicine when data is sparse. The key is to be aware of the evidence that exists and its limitations, to take pragmatic and proportional action based on what the research says, and to be flexible and prepared to change our practices as the evidence develops.
There is reason to believe all the effort and sacrifices we have made as a hospital, as well as that of government agencies, businesses, and individuals in our area, have been effective. Though Santa Clara County was one of the first centers of community spread of SARS-CoV-2 in the U.S., cases have not grown as fast here as in some other places, and the health-care system has so far been able to cope well with the number of COVID-19 patients (12, 13). We appear to be “flattening the curve,” a rather dry and abstract phrase that represents a meaningful reduction in human suffering.
As a hospital, we have been fortunate to not yet have any known cases of COVID-19 among our staff. However, the reality is that it is only a matter of time before someone we know is infected, or falls ill, or perhaps even dies as a result of this disease. The mitigation measures we have taken and have been imposed throughout our area and around the world are not sustainable in the long term. With a highly virulent virus spreading through a completely naïve population, no proven effective treatment, and a vaccine well over a year away by some estimates, the disruption this disease has brought to our hospital and our lives will persist and evolve for a long time to come.
However, we have also learned a great deal about our capabilities as individuals and as an organization. We have been reminded of the value of creating an adaptive, science-based practice culture and of the habits and methods of evidence-based medicine. We have learned from the ways in which we were prepared to cope with this unexpected crisis, and from the ways in which we weren’t. COVID-19 has reminded us of the essential nature of veterinary medicine, not only in companion animal health and food safety, but in human health as well. It would be difficult to find a more dramatic validation of the One Health concept than our current situation.
The months ahead, perhaps even years, will continue to be challenging because of this virus, but we have tools and knowledge not available during the last century that have allowed us to respond more quickly and effectively, and this has made a very real difference in the lives of millions of people. We can and should do better in the future at preventing, predicting, and responding to such public health threats, and with the lessons learned now, I have no doubt we will. My hope is that as a hospital community and as a profession, we will emerge from this crisis stronger, smarter, and better equipped to face such challenges in the future.

Would it be safe to board my dog if I became sick? I am in a high risk group but my dog is 17 years old with health issues so it seems like it would be better to board her in that case so that my family doesn’t have to care for her needs. She is not anxious at the vet so she would be fine there. Would a vet be able to board her for potentially a couple of weeks without risk to them?
As far as we know from the limited information currently available, the risk of coronavirus infecting dogs or being spread by dogs is extremely low, so it should be possible to safely care for her elsewhere if someone in the family develops COVID-19. The CDC recommendations for this situation are here. It would also depend, of course, on your local boarding facilities and their setup.
Good luck, and stay safe!
Silicon valley Elon musk likes these corona guys.
https://www.youtube.com/watch?v=zb6j7o1pLBw
when your back working full time ask your boss what he thinks about giving local vets in the area hospital privileges. If that will not work how about let them follow the specialist around. Got to be better CE than what required CE general practice vets are getting now at local meetings. If private hospitals cannot fill the demand I bet the Mars family will fill the demand. At least for vets who work for the family.
April 27, 2020
ACEP-AAEM Joint Statement on Physician Misinformation
The American College of Emergency Physicians (ACEP) and the American Academy of Emergency Medicine (AAEM) jointly and emphatically condemn the recent opinions released by Dr. Daniel Erickson and Dr. Artin Messihi. These reckless and untested musings do not speak for medical societies and are inconsistent with current science and epidemiology regarding COVID-19. As owners of local urgent care clinics, it appears these two individuals are releasing biased, non-peer reviewed data to advance their personal financial interests without regard for the public’s health.
COVID-19 misinformation is widespread and dangerous. Members of ACEP and AAEM are first-hand witnesses to the human toll that COVID-19 is taking on our communities. ACEP and AAEM strongly advise against using any statements of Drs. Erickson and Messihi as a basis for policy and decision making.
Unfortunately, these guys are fountains of misinformation and have actually drawn a rebuke from the emergency and critical care community for their nonsense.
I’m curious about your triage tool — are you having clients defer on things like noncore booster vaccinations at this point, for example?
Yes. We are continuing to provide initial vaccines for puppies, but no boosters for well pets at this time.
This has been really frustrating for me, with a working dog and breeding operation. Staff are usually not equipped to or capable of handling my dogs, and more than once procedures have been done to my dogs without my consent. When animals are a livelihood, there is no care that isn’t essential.
I almost lost a valuable (and much loved) young dog due to poor triage and slow response from an emergency vet (the only one) in my area who had similar procedures in place. I had to raise holy hell to get the dog into the clinic in time. This is just an ineffective way to do veterinary medicine, unfortunately. As you pointed out, most people (vets and staff) have other family members coming in and out of the home, so banning clients from the hospital is really not meaningful in the long run. I’m way more at risk from anyone working at a vet clinic than they are from me. It doesn’t make sense to me to refuse to use my own leash, but instead put a clinic leash on my animals, one that has been used on dozens and dozens of strangers’ animals, exposing me to whatever they had on their hands when they touched their dogs. I don’t like that the paranoia is only one-sided in such cases.
My continuity plan going forward is to find a way to hire an in house veterinarian, because I can’t afford the slip ups that keep happening with this way of operation.
I’m sorry you’ve had a bad experience. Most of our clients seem to feel the accommodations are working pretty well. As I’m sure you understand, no one planned for this, so everything is being invented on the fly. Contact with the public is a major risk factor, and it really makes no sense to suggest they are more a risk to you than you are to them. Any contact and interaction with other people is a risk, and the less of this there is the less community transmission will happen.
And for what it’s worth, all the vets and staff at our clinic are working harder and longer hours to try and continue providing services without putting ourselves or our family members at risk. Some inefficiency seems a reasonable price to pay for helping me not to bring COVID home to my 80 year-old mother.
Sorry for commenting on a bunch of your stuff – doing a late night read of your blog.
What are things looking like at your clinic, now, a year later? Are you still doing curbside service and are human clients still not allowed inside?
I try to be an understanding individual but it’s been over a year, we know a lot more about the virus, vaccines are a thing, and I feel like curbside needs to be over… yesterday.
Curious what things are like across the country in terms of that.
We are just beginning to let people back in the hospital with accommodations, so things are likely to change pretty rapidly over the next couple of months.
I’m now, more than a year after the last comment, wondering if what I’m finding at veterinary hospitals and clinics here in Georgia is true everywhere: care is damned hard to find.
I don’t fully understand what happened to clinic staff – where they went – but I’m told that staffing issues are the reason that even dogs who may have cancer are being told there’s a 3 month wait for an appointment at the state veterinary school small animal hospital – and a month or more wait at even the corporate-owned specialty hospitals.
My dog was determined to have a mass that “could be” lymphoma, and the wait to get her seen for further diagnosis was unbearable. Took more than a month to get her to a specialist after cytology was non-diagnostic and, in that time, she could’ve died from the lymphoma.
Fortunately, though we STILL don’t have a diagnosis, she’s still here and nearly symptom-free (with the exception of an occasional cough, which is why the mass was found in the first place), so we’re hopeful that means she does NOT have lymphoma. But it’s scary to find that veterinary care – from routine to emergency – is now so hard to find access to, even in a busy metropolitan area that’s replete with expensive specialty and general vets.
I have 2 senior dogs (the second/older one now also occasionally coughing!) and I took them into my home making the promise that they’d have good healthcare – and now I’m finding it harder to live up to that promise. I just don’t understand the issues behind why care has become so much less accessible, and don’t know if it’s pandemic-related, or something else.
Of course, these things are always complex and lots of factors are involved. Many industries in the U.S. are short-staffed now, due to the pandemic and the “Great Resignation.” Veterinary medicine was in trouble before the pandemic, but this has absolutely made things worse.
Here is an article that I thought summed up the problem as well as I’ve seen.