
I am preparing a series of lectures for an upcoming conference, and it has given me a chance to reflect on some of the core ideas that have always driven this blog– the challenges created by our human limitations and the strategies we have develop to mitigate them.
This lecture attempts to illustrate what evidence-based medicine is and, perhaps more importantly, why we need it. In this current Age of Endarkenment, when science is under attack and misinformation is rampant, such reflection is more important than ever.
Our Shared Malady
Evidence-based medicine (EBM) is a treatment for a disease most of us don’t realize we have. It is both a preventative and a treatment, really, but it is not a cure. The best we can hope for is to manage the symptoms and minimize the damage done by our disease.
The disease we suffer from lies in our brains. The mechanisms of observation and judgement we rely on as veterinarians to make recommendations for our patients are riddled with lesions. These have names like confirmation bias, cognitive dissonance, logical fallacy, and many others. The forms and manifestations of our disease are legion.1,2
The consequences of our illness are, sadly, experienced mostly by our patients. Misdiagnosis, overdiagnosis, rejection of effective therapies and use of ineffective ones, and ultimately suffering and death that could, perhaps, be avoided if we sought treatment for our condition.
Like many medicines, EBM, can be bitter and uncomfortable to take. Many of us don’t know we need it, and even when we are diagnosed we may reject the treatment as too unpleasant. And there are potential adverse effects from treatment. A clear understanding of our limitations can be overwhelming, leading to despair and even therapeutic nihilism. However, the potential benefits are great and worth the risks.
Before I describe the treatment, I need to characterize the disease and convince you that you have it. This is especially difficult because the features of our malady include elements specifically inhibiting our ability to recognize it. Confirmation bias blinds us to evidence of our illness. Cognitive dissonance causes pain when we are forced to see and acknowledge such evidence. The Dunning-Kruger effect makes those of us least knowledgeable about the illness feel the most confidence that we are free of it.
The best way to start on our journey may be with a story. Once there was a doctor, a kindly man who cared for children named Dr. Spock. He was an intelligent, caring doctor who brought great progress to the field of pediatrics and parenting. He wrote a book for parents called The Common Sense Book of Baby and Child Care,3 that sold millions of copies, was translated into 29 languages, and became a worldwide guide for parenting.
One key piece of advice Dr. Spock gave parents was that they should always put their babies to sleep on their stomach. Decades of experience, and simple common sense, showed Dr. Spock that doing so would reduce the risk of aspiration if an infant vomited, and this would help prevent Sudden Infant Death Syndrome (SIDS). SIDS is a terrifying and poorly understood condition in which apparently healthy babies die without warning, and parents are desperate for any action they can take to prevent it.
From the publication of Dr. Spock’s in 1946 until the early 1970s, the practice of putting infants to sleep on their stomachs was widely adopted, and parents were reassured by the confident recommendation of their doctors to follow this practice.
However, by the 1970s, abundant research had accumulated showing this practice was a mistake. Babies sleeping on their backs were actually more likely to die of SIDS.4 Despite this evidence, the practice persisted until the early 1990s. For twenty years, parents around the world did the wrong thing, even after science had showed it was wrong, because of cultural inertia, confidence in respected authorities, anecdotal experience, and all the other sources of our confidence in mistaken beliefs.
A review published in 2005 found that heeding the evidence and abandoning the traditional practice sooner might have saved the lives of 10,000 children in the U.K. and 50,000 in Europe, the U.S., and Australasia.4 When educational efforts finally reached parents, and they began putting babies to sleep on their backs, the rate of SIDS dropped markedly.

Figure 1. SIDS rate versus prone sleeping rate in the United States, 1983 to 1995 (from Carroll, 19985)
Does this mean Dr. Spock was a bad doctor? A fool? Were parents around the world stupid? No! This tragedy was a consequence of the illness we all suffer from- a natural tendency to see our personal observations and the stories told by others as compelling and reliable guides to reality, and a lack of a deep, effective appreciation of our limitations and the advantages of scientific data over anecdote and plausible reasoning.
Evidence-based medicine is “the conscientious, explicit, and judicious integration” of controlled research evidence with our clinical expertise and judgement and the goals and values of our clients.6,7 It is not a rejection of the value of the observations and judgements we make, but a recognition of their limitations and the dangers of trusting them too far. It is a set of methods and practices, yes, but first and foremost it is a philosophy, a perspective. “At its heart is the confidence in the scientific methodology that has developed over the centuries to enable us to distinguish what is likely to be true from what is likely to be false.”8 Diagnosing the illness, admitting we have a problem, is the necessary first step for starting treatment. I can teach you a bit about the treatment and how it works, but it won’t help you if you don’t begin by seeing that you need treatment.
Does EBM Work?
Proving that EBM is effective is not a simple matter. Where is the completely omniscient and objective observer who can judge that one approach to knowledge is better than another? Who would be willing to admit to practicing opinion-based medicine or belief-based medicine and then be willing to participate in a scientific study to show that their approach is better (or worse) than science?
The best we can do is make some logical inferences, though I personally think these are quite compelling. Consider the change in human life expectancy over time (Fig. 2)

Figure 2. Life expectancy around the world
While this chart starts in the 18th century, the available evidence suggests that the flat line, with overall life expectancy less than 40 years, could be extended many thousands of years into the past. Figure 3 shows a major reason for this, which is the high proportion of human children who did not survive to adulthood for most of human history.

Figure 3. Childhood mortality.
For the vast majority of human history, most humans didn’t survive childhood (or childbirth), and we were plagued with parasites and infectious diseases, malnutrition, and a host of other acute and chronic ills. While a lucky few in each generation managed to live to old age, the great majority could expect only the Hobbesian reality of a “poor, nasty, brutish, and short” life. And then, in a mere handful of centuries, that changed.
Today, we enjoy a length of life and a state of health and wellbeing unimaginable to even the most fortunate of our ancestors. What changed? Did we evolve physically? Did the environment become more hospitable? The gods kinder?
The answer is simple and profound- science. All that changed was our ability to understand nature. Over centuries, we developed the methods of scientific thought and practice that led to a more accurate understanding of the causes of illness and death. And with that improved understanding came both new techniques for treatment and prevention, and also new methods for testing those techniques.
We are using the same brains our ancestors used. In our daily life, including in clinical practice, we still observe and reason as they did, and we make all the same errors. But we defer often enough to the picture of reality built by the community of scientists using scientific methods that we end with better information and making better choices.
EBM is just an extension of this set of methods. The basic steps, and all the detail and nuance embedded in them, are all simply a practical application of the principles and methods of science to clinical practice. Deciding, then, whether EBM is worth using depends largely on deciding whether science is better than the alternatives that preceded it. The alternatives most propose—relying more on clinical experience, tradition, or reasoning from theoretical principles- are the same that guided medicine in all the centuries before the changes in figures 2 and 3 began.
The Basics of EBM
The core of EBM in practice is quite simple. It consists of five basic steps-
- Ask a question
- Locate relevant evidence
- Evaluate this evidence
- Draw a conclusion
- Assign a level of confidence
These steps are repeated as often as necessary until we feel we know enough to take action. They are repeated again whenever we have new questions, new evidence appears, or new action is needed. Entire textbooks have been written to guide us through these steps, but the basic process comes down to this.
The Question
The first step is to identify what we need to know to care for a given patient. What tests should we run? What treatment should we use? How can we tell if the treatment is working? What can we tell the owner about risks or prognosis?
The key to getting useful answers from the scientific literature is asking useful questions. They should be specific enough to turn up relevant evidence but not so narrow that we exclude useful information. “Do antibiotics work?” is too broad to be meaningful. “Should we use amoxicillin, cephalexin, or enrofloxacin, for one week or for two weeks, in a 9 year-old neutered male Labrador retriever with an infected laceration from a stick on the front limb?” is not going to turn up many relevant clinical studies. Learning how to organize or ignorance and structure our questions is an EBM skill that can be developed, and there are many resources to support this.
Finding the Evidence
Another critical EBM skill is learning how to locate useful evidence. Sources as varied as textbooks, scientific journals, online databases and discussion forums, and even the vet working in the office next door are all available, and they all have their strengths and weaknesses. The best evidence is often the scarcest and hardest to access, while the most convenient sources often come with the greatest limitations. Locating and acquiring evidence requires us to be a bit like a detective or someone on a scavenger hunt, which can be fun but can also take time we don’t have. Building a collection of skills and resources over time can reduce the burden of finding useful evidence.
Evaluating the Evidence
It would be ideal if we could simply read a published scientific study or listen to the advice of our colleagues and immediately put the information we find into practice. Unfortunately, not all evidence is equally reliable, and even high-quality data may not apply to the patient in front of us. Critical appraisal of evidence is arguably the most important, and the least used step in this list.
There are shortcuts that can help us. The classic pyramid of evidence in Figure 4 illustrates an approach to evidence that is sophisticated but academic and not always useful in practice.
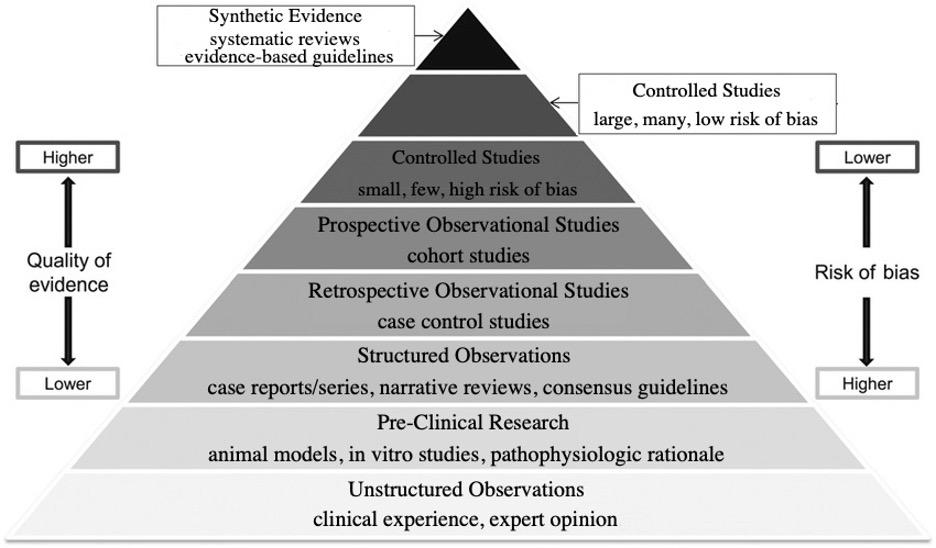
Figure 4. Traditional evidence pyramid.
I prefer a simpler scheme which is more easily applied for most of us.
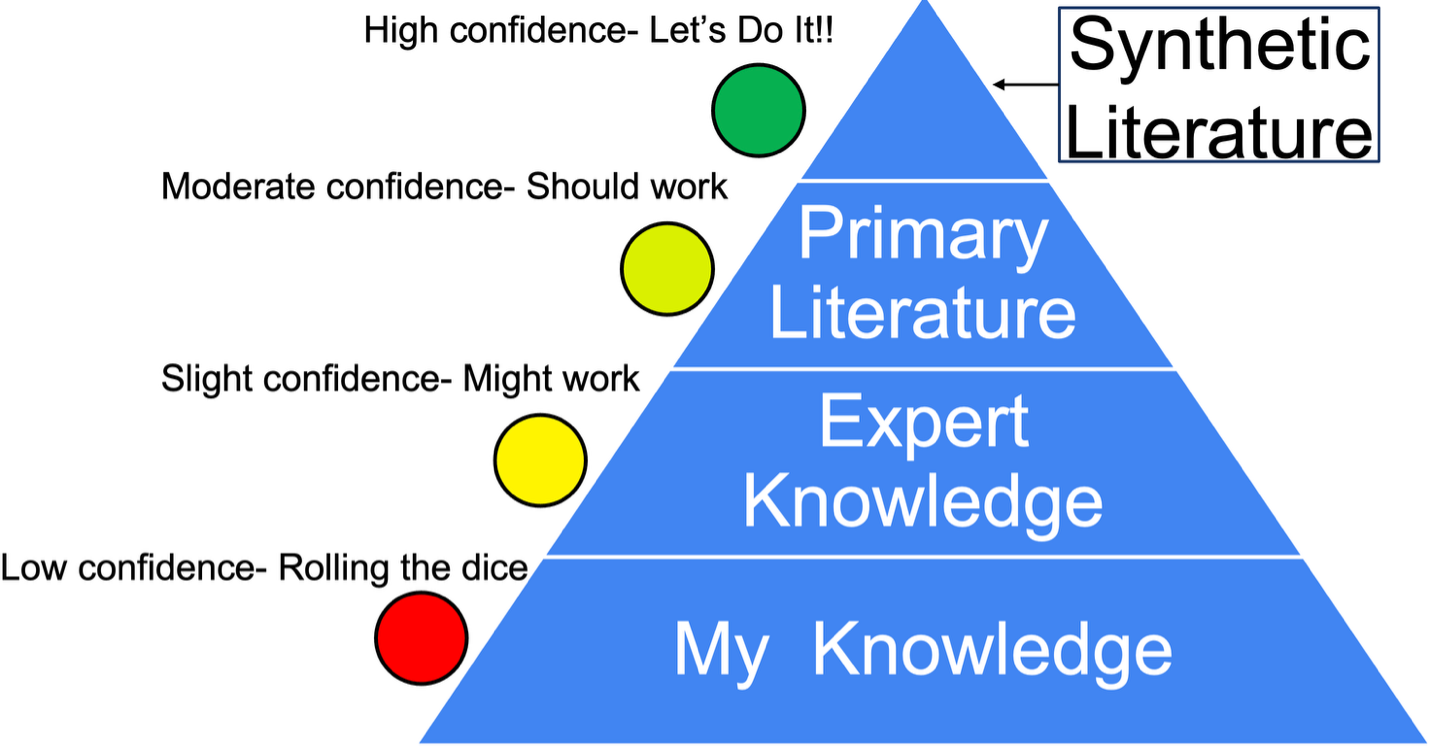
Figure 5. Practical evidence pyramid.
This emphasizes that all sources of evidence are potentially useful, but the closer we get to the top of the pyramid, the more confidence we can have in the information. Synthetic resources, such as clinical practice guidelines and systematic reviews, are especially valuable since they are both high in reliability and efficient, requiring less time, effort, and expertise to use effectively.
The Conclusion and the Confidence
Once we have gathered the available evidence and evaluated it, our main job is to decide what it means. What actions should we take or avoid based on the evidence? Just as important as the conclusion we reach is the level of confidence we assign to it. If I choose to say, “Here is a powerful therapy which will cure your cat,” that sets up very different expectations and behavior, in the owner and in myself, than if I say, “Here’s a therapy a few people have tried in dogs that might help your cat.” For reasons both practical and ethical, it is crucial that we choose and communicate an appropriate level of confidence for the recommendations we make.
Our disease drives us to have confidence greater than warranted by most of the evidence we are likely to have available. EBM gives us both a warning and some techniques for setting a more appropriate level, which then encourages more truly informed consent from our clients and probably more reasonable expectations and better followup.
The Madness and Wisdom of Crowds
Let us end with another story. On a cold Thursday morning in December, 1799, the former president of the United States, George Washington, rode out into the snow to inspect his farmlands.9 He was 68 years old, but strong and healthy for his age. That night he developed a bit of a sore throat, and by a day later he was having a hard time breathing.
Unable to swallow a remedy of vinegar, molasses, and butter due to swelling in his throat, he accepted his doctor’s suggestion to remove a half pint (about 240mls) of blood from his arm. The patient did not improve, and the procedure was repeated several times over the day, with various doctors removing a total of about 3 to 4L of blood (about a third to half of the typical total blood volume for an adult man). Despite these heroic efforts, the former president died after about 13 hours of intensive treatment.
Bloodletting has been a routine and respected therapy in many cultures around the world and in many different historical eras. It is based on a simple powerful idea: What if we all illness stemmed from a derangement of a few essential factors, and we could prevent or cure illness simply by keeping these in balance?
This idea is intuitively appealing, clear, and logical. It is also, of course, wrong. But every time it has emerged, it has captured the imagination and deep faith of the brightest medical and scientific minds, and persisted for centuries, even millennia, and into the present day.
A reasonable catchall name for this view is humorism. It was the rationale for the treatment of bloodletting promoted by Hippocrates in the 5th century BCE and accepted by George Washington’s doctors in 1799. Some versions of humorism persist today in the theories of Traditional Chinese Medicine and Indian Ayurveda.
There have always been skeptics of bloodletting. George Washington’s wife opposed the practice and begged his doctors not to take so much blood from her husband. But the logic of humorism and the innumerable anecdotes of patients cured by the practice overcame such skepticism. As late as 1875, defenders of the practice argued for it with reference to such compelling evidence:
“Who is there with ten or twenty years experience in the profession, that has not seen the most marked advantages from bleeding…” asked one such defender.10 Another learned physician wrote that, “He thought it really saying too much…that we should assume to be so much wiser than our fathers, who had lent their approval to a custom that had been sanctioned by ages of experience.”10
Eventually, the current models of physiology and disease replaced humorism, and the methods of science replaced bloodletting with a range of practices that, while imperfect, have nearly doubled human life expectancy and brought levels of health and comfort unimaginable in most of human history.
So were all our “fathers” bad doctors? Fools? No! This story is meant to show the unique and challenging nature of our disease. It is both congenital, built into each of our brains from birth, and also communicable. The manifestations of this illness in each of us magnifies the symptoms in others, and in a population the disease can make us sicker and do more harm that in one isolated patient. We can reinforce and sustain each other’s beliefs, even if they are egregiously wrong.
Fortunately, the same power of the community lies in the treatment for our illness. Science is a community process in which we pit our limited, imperfect, biased notions against each other in a competition judged by the strength and consistency of the data we can produce. Though the madness of crowds11 can lead us horribly astray, the wisdom of crowds12 can rescue us from our individual delusions. The secret is to harness the competition of ideas in a race governed by the rules and standards of science and evidence.
Evidence-based medicine is a part of the larger project of using science to control our illness, to keep us closer to the truth of nature so we can help our patients most effectively.
Key Points
- Human observation and judgement is inherently flawed, and our confidence in our reasoning is typically greater than the true accuracy of our beliefs.
- Evidence-based medicine (EBM) is a facet of the greater project of science. It is a set of perspectives and practices meant to improve the accuracy of our understanding of nature and set appropriate degrees of confidence around our beliefs.
- The five basic steps of the EBM method are-
- Ask a question
- Locate relevant evidence
- Evaluate this evidence
- Draw a conclusion
- Assign a level of confidence
This is an iterative process, repeated often as our information needs and the available evidence change.
- Groups of humans can strengthen and persist in false beliefs for generations.
- Groups of humans can also develop more accurate understanding of nature if guided by the methods of science
- Individual clinicians can benefit from EBM by
- Maintaining an awareness of our disease and its consequences
- Following the steps of EBM
- Relying on the work of a scientific community more than on individual personal experience and belief
References
1. Kida T. Don’t Believe Everything You Think. Prometheus; 2006. Accessed October 9, 2025. https://www.simonandschuster.com/books/Dont-Believe-Everything-You-Think/Thomas-E-Kida/9781591024088
2. McKenzie BA. Veterinary clinical decision-making: cognitive biases, external constraints, and strategies for improvement. J Am Vet Med Assoc. 2014;244(3):271-276. doi:10.2460/javma.244.3.271
3. Spock B. The Common Sense Bookf of Baby and Child Care. 1st ed. Duell, Sloan, ad Pearce; 1946.
4. Gilbert R, Salanti G, Harden M, See S. Infant sleeping position and the sudden infant death syndrome: systematic review of observational studies and historical review of recommendations from 1940 to 2002. Int J Epidemiol. 2005;34(4):874-887. doi:10.1093/ije/dyi088
5. Carroll JL, Siska ES. SIDS: counseling parents to reduce the risk. Am Fam Physician. 1998;57(7):1566-1572.
6. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312(7023):71-72. doi:10.1136/bmj.312.7023.71
7. Straus SE, Glasziou P, Richardson WS, Haynes RB. Evidence-Based Medicine: How to Practice and Teach EBM. 5th ed. Elsevier; 2019.
8. Cockroft PD, Holmes MA. Handbook of Evidence-Based Veterinary Medicine. Blackwell; 2003.
9. Vadakan V. The Asphyxiating and Exsanguinating Death of President George Washington. In: 2004. Accessed October 9, 2025. https://www.semanticscholar.org/paper/The-Asphyxiating-and-Exsanguinating-Death-of-George-Vadakan/33f243e97580948b73e700df9489906a37849247
10. McKenzie BA. Placebos for Pets?: The Truth About Alternative Medicine in Animals. Ockham Publishing; 2019.
11. Mackay C. Extraordinary Popular Delusions and the Madness of Crowds. chard Bentley; 1841.
12. Surowiecki J. The Wisdom of Crowds. First Anchor books edition. Anchor Books, a division of Random House, Inc; 2005. Accessed October 9, 2025. http://catdir.loc.gov/catdir/samples/random051/2003070095.html

I may be old school. I’m not convinced the new EBM medicine pyramid is little more than an attempt to mix cow pie with apple pie to promote selling treatments without two good independent randomized controlled trials that prove efficacy. Sham surgeries can be done. If something works, it can be proven to work. We do not need to know why it work but I think proof it works is needed unless you want to pull out the parachute argument card that you do not need a RCT to prove you need a parachute when jumping out of an airplane. The evidence-based medicine (EBM) pyramid has evolved significantly since its early depictions in the 1990s, when systematic reviews (often of randomized controlled trials, or RCTs) were prominently placed at the top, with RCTs just below, followed by cohort studies, case-control studies, case series, and expert opinion at the base. Traditional Pyramid Early versions explicitly highlighted systematic reviews of RCTs as the highest level of evidence and RCTs as a key mid-to-high tier due to their perceived low risk of bias.Key Change in 2016A influential perspective published in BMJ Evidence-Based Medicine (Murad et al., 2016) proposed a “new evidence pyramid” that reframed the role of systematic reviews and meta-analyses. The authors argued that while systematic reviews synthesize evidence effectively, they are not inherently the “highest” form of evidence themselves.
We’ve argued about this before, and it comes down to the difference between evidence-based medicine and science-based medicine. There’s plenty of Tooth Fairy science out there, and you can do all the RCTs you want for homeopathy, but it is still mystical nonsense that doesn’t work. The RCT is a very important and useful type of evidence, but it is not perfect and it is capable of misleading us. It is also often not possible even when desired, and yet we have to make decisions and do things for patients, so we need a comprehensive approach to assessing evidence that doesn’t focus only on RCTs.