I recently updated my coverage of attempts by the American College of Veterinary Botanical Medicine (ACVBM) to attain specialty recognition, and explained why I am opposed to this effort. The deliberations and decisions of the American Board of Veterinary Specialties (ABVS) are shrouded in mystery and seldom discussed publicly, but I have been able to confirm that the ABVS has rejected the ACVBM petition. While I am hopeful that appropriate scientific study will find useful treatments buried in the pile of accumulated tradition and anecdote that currently makes up veterinary herbal medicine, I believe the ACVBM is not the organization to lead this effort, and I think the ABVS decision is in the best interests of animal patients.
Since the late 1980s, individuals and organizations have been trying to warn the public about a deadly chemical known as DHMO. Though widely used in the home and in commercial settings, including the healthcare industry, this substance has been shown to cause severe lung damage and even death if inhaled in small quantities. Hundreds of thousands of people die annually from this cause.1
DHMO can also cause electrolyte disturbances and potentially fatal neurologic symptoms when taken orally, and it can cause severe burns and even explosions when heated.2A number of surveys have found high levels of support for banning DHMO, and elected officials in several countries have explored taking such action, but DHMO remains ubiquitous.3,4
Given the obvious dangers of this chemical, why do public health agencies not take action to restrict it? It is possible that funding and political influence from industry impedes regulatory action. However, it is more likely that governments have chosen not to ban DHMO because it is essential for life. Most people are surprised to learn this until they recognize the non-technical name for this chemical—water.
The campaign against DHMO (dihydrogen monoxide) has been used as a humorous illustration of the problem of chemophobia or chemonoia. These terms refer to the potent and widespread fear of anything labeled a “chemical.”5–7Nonscientists often assume that chemicals are inherently dangerous, even though the word properly refers to nearly every substance we encounter in daily life, from the deadliest poison to the basic necessities of life and even the materials that makes up our own bodies.
A concept integral to chemophobia is the Appeal to Nature Fallacy, the misconception that substances which occur naturally are inherently healthy and safe while those produced by humans, even if chemically identical to natural substances, are dangerous. Of course, it is easy to find examples that belie this notion. Nothing could be more natural than the E. colior Salmonella. Radioactive uranium, asbestos, and cyanide are completely natural.
In contrast, the vaccines which have eliminated smallpox and polio are undeniably artificial. Antibiotics, synthetic vitamin supplements, blood transfusions, organ transplants, prosthetic limbs, insulin for diabetics, and even such simple and unheralded public health technologies as indoor plumbing and toilet paper have saved lives and reduced suffering for millions. Yet these are not “natural” in the usual sense of the word.
Unfortunately, chemophobia and the Appeal to Nature Fallacy are widespread, and they often motivate pet care decisions. Some organizations and individuals take advantage of this by offering “natural” products or therapies and warning of the dangers of “chemicals” and anything “artificial.” A recent high-profile example of this exploitation of chemophobia is the announcement by Petco that the company “will not sell food and treats containing artificial colors, flavors and preservatives for dogs and cats.”8
The company’s public relations materials call this decision “a major step forward for pets” on “a momentous day.”8Petco effectively declares itself the arbiter of what constitutes healthy nutrition, even going so far as offering to “help pet parents affected by such a change to safely transition to a new food or brand that we believe is healthier for their pet” if customers are no longer able to buy a food they have been using.8Even though regulatory agencies and experts around the world have judged the additives on Petco’s list to be safe, the company has decided it knows better.
The dramatic rhetoric in the Petco press materials may serve the purpose of creating a positive and profitable image for the company, but it obscures the danger of a marketing strategy that caters to unscientific reasoning and mostly unfounded fears. There is little in the way of scientific evidence, or even logical consistency, behind the Petco blacklist.9
For example, many of the “artificial” flavors and preservatives on the list occur naturally (see Table 1). Of course, the fact that these chemicals occur in nature doesn’t make them safe, just as flavors and preservatives are not necessarily unsafe if produced synthetically. However, the fact that Petco is banning naturally occurring substances for being “artificial” exposes the inconsistent logic behind this blacklist.
The health risks of most substances are related to the dose and route of exposure. And the risk of any substance should always be considered in relation to its benefits. Water is unsafe to drink only in very large quantities, but it is unsafe to breathe in even small amounts. It is also essential for life, taken at appropriate doses and by the appropriate route. The same logic, informed by scientific evidence concerning risks and benefits, should be applied to food additives, but Petco does not use this approach.
Some of the substances on the list have no clear health implications. The color additives, for example, are almost certainly safe, but they serve no nutritional or health purpose.10,11,20–25,12–19These chemicals are added to pet food to appeal to the emotions and aesthetics of pet owners. While they serve no health-related purpose, banning these compounds is itself a way of appealing to the emotions of owners and their irrational fears, and there is no sound reason to believe this will benefit the health of pets.
For other items on the list, the impact of discouraging their use is less clear. Flavorings, for example, make nutritious and affordable commercial foods more palatable. Removing them may make it harder to provider appropriate nutrition to pets, and it may encourage owners to switch to homemade or other alternative diets that are often nutritionally inferior.26–31
The most clearly beneficial chemicals on the blacklist are the preservatives. Preventing spoilage, pathogen growth, and loss of nutrients in pet food is critical to providing healthy diets. In the absence of convincing evidence that commonly used and legally approved preservatives are actually harmful, removing them can only lead to less safe and healthy food for pets.
The evidence of health risks for most of the additives on the list is weak and based primarily on in vitroand lab animal studies that do not reliably predict the effects of normal use in pet foods. Most of these additives have been used for decades and reviewed periodically by regulators with no convincing evidence of negative health effects in humans or pets. Some may have risks that warrant removing them from use, but the evidence to make this case is lacking.
One can make the argument, of course, that any substance which has shown any hint of toxicity in lab animal studies ought to be avoided. There is little evidence, however, that this precautionary approach actually reduces harm. If the substances that are abandoned are actually safe, then there is no benefit. And there is always the potential that new, less thoroughly tested alternatives may have greater risks, even if they are “natural.”32
There is even evidence that some of the additives on the Petco list may actually have health benefits (see references from Table 1). Many have antiseptic, anti-inflammatory, anti-neoplastic, and antioxidant activity or other potentially beneficial uses. While the evidence for these effects is weak and based mostly on in vitroand lab animal studies, this is no less convincing than the evidence for negative health effects Petco has used to justify banning these compounds.
Irrational and unscientific reasoning is not likely to lead to good healthcare choices. Unjustified fear of grains has led to grain-free diets making up about 25% of the dog food market. There is no reason to believe these diets have health benefits, and there are beginning to be signs that feeding these diets may be harming dogs.33–35The same reasoning that underlies this blacklist has also led Petco to sell raw diets, which have well-established health risks,28,36–42and to offer worthless homeopathic remedies43–47that pet owners may mistakenly substitute for effective, science-based medical treatment.
The best way to protect our pets’ health is to rely on sound scientific evidence to help us weigh the risks and benefits of the food and medicine we provide, not to cater to irrational fears like chemophobia and meaningless distinctions such as “natural” and artificial.” Table 1 provides a partial list of the sources, regulatory approvals, and evidence for safety and potentially beneficial effects of the items on the Petco blacklist. This is not a comprehensive review, simply an illustration that the items on this list are often “natural,” are judge by government experts around the world to be safe as used in food for humans and animals, and may have beneficial uses that offset any risk they may present.
Veterinarians have a responsibility to support and educate pet owners and to challenge unscientific, fear-based marketing ploys like the Petco blacklist. The movement towards dangerous “natural” practices like feeding raw diets and avoiding vaccination is a real threat to animal welfare, and it is exacerbated by companies seeking market advantage through feeding and capitalizing on misconceptions and fear.
References
1. World Health Organization. Drowning.; 2018. https://www.who.int/news-room/fact-sheets/detail/drowning. Accessed December 24, 2018.
2. DHMO.ORG. Facts About Dihydrogen Monoxide. http://www.dhmo.org/facts.html. Published 2018. Accessed December 24, 2018.
3. DHMO.ORG Research Division. DHMO Research Reports. http://www.dhmo.org/research.html. Published 2008. Accessed December 24, 2018.
4. Stuff.co.nz. National MP falls victim to water hoax. Stuff. http://www.stuff.co.nz/national/politics/38005/National-MP-falls-victim-to-water-hoax. Published 2009. Accessed December 24, 2018.
5. Robson D. Chemonoia: The fear blinding our minds to real dangers. BBC FUture.
6. Francl M. How to counteract chemophobia. Nat Chem. 2013;5(6):439-440. doi:10.1038/nchem.1661
7. Ropeik D. On the roots of, and solutions to, the persistent battle between “chemonoia” and rationalist denialism of the subjective nature of human cognition. Hum Exp Toxicol. 2015;34(12):1272-1278. doi:10.1177/0960327115603592
8. Petco. Petco First and Only Major Retailer of Pet Food to Not Sell Food and Treats with Artificial Ingredients. PR Newswire. https://www.prnewswire.com/news-releases/petco-first-and-only-major-retailer-of-pet-food-to-not-sell-food-and-treats-with-artificial-ingredients-300748831.html. Published 2018. Accessed December 24, 2018.
9. Ingredients Which Do Not Meet Petco’s New Nutritional Standards. https://www.petco.com/shop/en/petcostore/c/betternutrition-ingredients. Published 2018. Accessed December 24, 2018.
10. Bastaki M, Farrell T, Bhusari S, Bi X, Scrafford C. Estimated daily intake and safety of FD&C food-colour additives in the US population. Food Addit Contam Part A. 2017;34(6):891-904. doi:10.1080/19440049.2017.1308018
11. Bastaki M, Farrell T, Bhusari S, Pant K, Kulkarni R. Lack of genotoxicity in vivo for food color additive Allura Red AC. Food Chem Toxicol. 2017;105:308-314. doi:10.1016/j.fct.2017.04.037
12. Bastaki M, Farrell T, Bhusari S, Pant K, Kulkarni R. Lack of genotoxicity in vivo for food color additive Tartrazine. Food Chem Toxicol. 2017;105:278-284. doi:10.1016/j.fct.2017.04.034
13. Amchova P, Kotolova H, Ruda-Kucerova J. Health safety issues of synthetic food colorants. Regul Toxicol Pharmacol. 2015;73(3):914-922. doi:10.1016/j.yrtph.2015.09.026
14. Oplatowska-Stachowiak M, Elliott CT. Food colors: Existing and emerging food safety concerns. Crit Rev Food Sci Nutr. 2017;57(3):524-548. doi:10.1080/10408398.2014.889652
15. Younes M, Aggett P, Aguilar F, et al. Evaluation of four new studies on the potential toxicity of titanium dioxide used as a food additive (E 171). EFSA J. 2018;16(7). doi:10.2903/j.efsa.2018.5366
16. European Food Safety Authority (EFSA). Food colours: titanium dioxide marks re-evaluation milestone |. http://www.efsa.europa.eu/en/press/news/160914. Published 2016. Accessed December 25, 2018.
17. Food and Drug Administration (FDA). Titanium Dioxide.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfCFR/CFRSearch.cfm?fr=73.575. Accessed December 25, 2018.
18. European Food Safety Authority (EFSA). Food Colours. http://www.efsa.europa.eu/en/topics/topic/food-colours. Published 2016. Accessed December 25, 2018.
19. Food Standards Australia New Zealand. Food Colours. http://www.foodstandards.gov.au/consumer/additives/foodcolour/pages/default.aspx. Published 2012. Accessed December 25, 2018.
20. Food Standards Australia New Zealand (FSANZ). Supplementary food colours report. http://www.foodstandards.gov.au/science/surveillance/pages/supplementaryfoodcol5571.aspx. Published 2012. Accessed December 25, 2018.
21. FDA. Overview of Food Ingredients, Additives & Colors. US Food Drug Adm. 2010. https://www.fda.gov/food/ingredientspackaginglabeling/foodadditivesingredients/ucm094211.htm#qahyper. Accessed December 25, 2018.
22. Center for Food Safety and Applied Nutrition F. Food Additives & Ingredients – Color Additives Questions and Answers for Consumers. https://www.fda.gov/food/ingredientspackaginglabeling/foodadditivesingredients/ucm488219.htm. Accessed December 25, 2018.
23. Laflamme D, Izquierdo O, Eirmann L, Binder S. Myths and Misperceptions About Ingredients Used in Commercial Pet Foods. Vet Clin North Am Small Anim Pract. 2014;44(4):689-698. doi:10.1016/j.cvsm.2014.03.002
24. Wortinger A. Nutritional Myths. J Am Anim Hosp Assoc. 2005;41(4):273-276. doi:10.5326/0410273
25. Case LP, Daristotle L, Hayek L, Foess Raasch M. Common Nutrition Myths and Feeding Practices. In: Canine and Feline Nutrition. 3rd ed. Maryland Hwights, MO: Mosby Elsevier; 2010:277-294.
26. Weeth LP. Focus on nutrition: Home-prepared diets for dogs and cats. Compend Contin Educ Vet. 2013;35(3):E3. http://www.ncbi.nlm.nih.gov/pubmed/23532921. Accessed October 28, 2018.
27. Streiff EL, Zwischenberger B, Butterwick RF, Wagner E, Iben C, Bauer JE. A Comparison of the Nutritional Adequacy of Home-Prepared and Commercial Diets for Dogs. J Nutr. 2002;132(6):1698S-1700S. doi:10.1093/jn/132.6.1698S
28. Schlesinger DP, Joffe DJ. Raw food diets in companion animals: a critical review. Can Vet J = La Rev Vet Can. 2011;52(1):50-54. http://www.ncbi.nlm.nih.gov/pubmed/21461207. Accessed October 28, 2018.
29. Streiff EL, Zwischenberger B, Butterwick RF, Wagner E, Iben C, Bauer JE. A comparison of the nutritional adequacy of home-prepared and commercial diets for dogs. J Nutr. 2002;132(6 Suppl 2):1698S-700S. doi:10.1093/jn/132.6.1698S
30. Stockman J, Fascetti AJ, Kass PH, Larsen JA. Evaluation of recipes of home-prepared maintenance diets for dogs. J Am Vet Med Assoc. 2013;242(11):1500-1505. doi:10.2460/javma.242.11.1500
31. Hutchinson D, Freeman LM, McCarthy R, Anastasio J, Shaw SP, Sutherland-Smith J. Seizures and severe nutrient deficiencies in a puppy fed a homemade diet. J Am Vet Med Assoc. 2012;241(4):477-483. doi:10.2460/javma.241.4.477
32. Simon JE, Decker EA, Ferruzzi MG, et al. Establishing Standards on Colors from Natural Sources. J Food Sci. 2017;82(11):2539-2553. doi:10.1111/1750-3841.13927
33. Freeman LM, Stern JA, Fries R, Adin DB, Rush JE. Diet-associated dilated cardiomyopathy in dogs: what do we know? J Am Vet Med Assoc. 2018;253(11):1390-1394. doi:10.2460/javma.253.11.1390
34. Kaplan JL, Stern JA, Fascetti AJ, et al. Taurine deficiency and dilated cardiomyopathy in golden retrievers fed commercial diets. Loor JJ, ed. PLoS One. 2018;13(12):e0209112. doi:10.1371/journal.pone.0209112
35. Adin D, DeFrancesco TC, Keene B, et al. Echocardiographic phenotype of canine dilated cardiomyopathy differs based on diet type. J Vet Cardiol. 2019;21:1-9. doi:10.1016/J.JVC.2018.11.002
36. Freeman LM, Chandler ML, Hamper BA, Weeth LP. Current knowledge about the risks and benefits of raw meat-based diets for dogs and cats. J Am Vet Med Assoc. 2013;243(11):1549-1558. doi:10.2460/javma.243.11.1549
37. Health England P. Investigation into an Outbreak of Shiga Toxin Producing Escherichia Coli.; 2017. www.facebook.com/PublicHealthEngland. Accessed December 6, 2018.
38. Chengappa MM, Staats J, Oberst RD, Gabbert NH, McVey S. Prevalence of Salmonellain Raw Meat used in Diets of Racing Greyhounds. J Vet Diagnostic Investig. 1993;5(3):372-377. doi:10.1177/104063879300500312
39. Finley R, Ribble C, Aramini J, et al. The risk of salmonellae shedding by dogs fed Salmonella-contaminated commercial raw food diets. Can Vet J = La Rev Vet Can. 2007;48(1):69-75. http://www.ncbi.nlm.nih.gov/pubmed/17310625. Accessed October 27, 2018.
40. Joffe DJ, Schlesinger DP. Preliminary assessment of the risk of Salmonella infection in dogs fed raw chicken diets. Can Vet J = La Rev Vet Can. 2002;43(6):441-442. http://www.ncbi.nlm.nih.gov/pubmed/12058569. Accessed October 27, 2018.
41. Weese JS, Rousseau J, Arroyo L. Bacteriological evaluation of commercial canine and feline raw diets. Can Vet J = La Rev Vet Can. 2005;46(6):513-516. http://www.ncbi.nlm.nih.gov/pubmed/16048011. Accessed October 27, 2018.
42. Strohmeyer RA, Morley PS, Hyatt DR, Dargatz DA, Scorza AV, Lappin MR. Evaluation of bacterial and protozoal contamination of commercially available raw meat diets for dogs. J Am Vet Med Assoc. 2006;228(4):537-542. doi:10.2460/javma.228.4.537
43. Ernst E. Homeopathy – The Undiluted Facts. Cham: Springer International Publishing; 2016. doi:10.1007/978-3-319-43592-3
44. Ernst E. A systematic review of systematic reviews of homeopathy. Br J Clin Pharmacol. 2002;54(6):577-582. http://www.ncbi.nlm.nih.gov/pubmed/12492603. Accessed November 12, 2018.
45. Shang A, Huwiler-Müntener K, Nartey L, et al. Are the clinical effects of homoeopathy placebo effects? Comparative study of placebo-controlled trials of homoeopathy and allopathy. Lancet (London, England). 2005;366(9487):726-732. doi:10.1016/S0140-6736(05)67177-2
46. Ernst E, Pittler MH. Re-analysis of previous meta-analysis of clinical trials of homeopathy. J Clin Epidemiol. 2000;53(11):1188. http://www.ncbi.nlm.nih.gov/pubmed/11186614. Accessed November 12, 2018.
47. Ernst E. Classical homoeopathy versus conventional treatments: a systematic review. 1999. https://www.ncbi.nlm.nih.gov/books/NBK67846/. Accessed November 12, 2018.
48. Feron VJ, Til HP, de Vrijer F, Woutersen RA, Cassee FR, van Bladeren PJ. Aldehydes: occurrence, carcinogenic potential, mechanism of action and risk assessment. Mutat Res. 259(3-4):363-385. http://www.ncbi.nlm.nih.gov/pubmed/2017217. Accessed December 25, 2018.
49. ACETALDEHYDE WORKING GROUP Comments on the CLH Report on Acetaldehyde; Proposal for Harmonised Classification and Labeling (June 2015). https://echa.europa.eu/documents/10162/b9885f2c-b491-4ad4-8900-8cba349b15a0. Accessed December 25, 2018.
50. Evaluation Report of Food Additives Acetaldehyde Food Safety Commission Evaluation Results on the Health Risk Assessment of Acetaldehyde as Food Additive.; 2005. http://www.fsc.go.jp/english/evaluationreports/foodadditive/acetaldehyde_report.pdf. Accessed December 25, 2018.
51. Food and Drug Administration (FDA). Substances Generally Recognized as Safe.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfCFR/CFRSearch.cfm?fr=182.60. Accessed December 25, 2018.
52. World Health Organization (WHO). Evaluations of the Joint FAO/WHO Expert Committee on Food Additives (JECFA). http://apps.who.int/food-additives-contaminants-jecfa-database/search.aspx. Published 2017. Accessed December 25, 2018.
53. V. V. The Asphyxiating and Exsanguinating Death of President George Washington. Perm J. 2004;8(2):2002-2005.
54. Aguilar F, Nybro Autrup H, Barlow S, et al. Flavouring Group Evaluation 11, Revision 1 (FGE.11Rev1) 1 Aliphatic Dialcohols, Diketones, and Hydroxyketones from Chemical Group 10 Scientific Opinion of the Panel on Food Additives, Flavourings, Processing Aids and Materials in Contact with Food (AFC) PANEL MEMBERS. Vol 493.; 2008. http://www.efsa.europa.eu/sites/default/files/scientific_output/files/main_documents/493.pdf. Accessed December 25, 2018.
55. Xiao Z, Lu JR. Generation of Acetoin and Its Derivatives in Foods. 2014. doi:10.1021/jf5013902
56. Almodares A, Ranjbar M, Hadi MR. Effects of nitrogen treatments and harvesting stages on the aconitic acid, invert sugar and fiber in sweet sorghum cultivars. J Environ Biol. 2010;31(6):1001-1005. http://www.ncbi.nlm.nih.gov/pubmed/21506489. Accessed December 25, 2018.
57. Food and Drug Administration (FDA). Aconitic Acid.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=184.1007. Accessed December 25, 2018.
58. Aprotosoaie AC, Costache I-I, Miron A. Anethole and Its Role in Chronic Diseases. In: Advances in Experimental Medicine and Biology. Vol 929. ; 2016:247-267. doi:10.1007/978-3-319-41342-6_11
59. Aquilina G, Bories G, Chesson A, et al. Scientific Opinion on the safety and efficacy of allylhydroxybenzenes (chemical group 18) when used as flavourings for all animal species 1 EFSA Panel on Additives and Products or Substances used in Animal Feed (FEEDAP). EFSA J. 2011;9(12):2440. doi:10.2903/j.efsa.2011.2440
60. Kim KY, Lee HS, Seol GH. Anti-inflammatory effects of trans -anethole in a mouse model of chronic obstructive pulmonary disease. Biomed Pharmacother. 2017;91:925-930. doi:10.1016/j.biopha.2017.05.032
61. Scott HR, Scott LE. Process of treating nut kernels to produce food ingredients. July 1920. https://patents.google.com/patent/US1416128. Accessed December 25, 2018.
62. Adams TB, Cohen SM, Doull J, et al. The FEMA GRAS assessment of benzyl derivatives used as flavor ingredients. Food Chem Toxicol. 2005;43(8):1207-1240. doi:10.1016/J.FCT.2004.11.014
63. da Silva DS, da Silva CEH, Soares MSP, et al. Thiazolidin-4-ones from 4-(methylthio)benzaldehyde and 4-(methylsulfonyl)benzaldehyde: Synthesis, antiglioma activity and cytotoxicity. Eur J Med Chem. 2016;124:574-582. doi:10.1016/j.ejmech.2016.08.057
64. Jang TY, Park C-S, Kim K-S, Heo M-J, Kim YH. Benzaldehyde suppresses murine allergic asthma and rhinitis. Int Immunopharmacol. 2014;22(2):444-450. doi:10.1016/j.intimp.2014.07.029
65. Final Report on the Safety Assessment of Benzaldehyde1. Int J Toxicol. 2006;25(1_suppl):11-27. doi:10.1080/10915810600716612
66. Heidor R, Ortega JF, de Conti A, Ong TP, Moreno FS. Anticarcinogenic actions of tributyrin, a butyric acid prodrug. Curr Drug Targets. 2012;13(14):1720-1729. http://www.ncbi.nlm.nih.gov/pubmed/23140283. Accessed December 25, 2018.
67. Sossai P. Butyric acid: what is the future for this old substance? Swiss Med Wkly. 2012;142:w13596. doi:10.4414/smw.2012.13596
69. McNabney SM, Henagan TM. Short Chain Fatty Acids in the Colon and Peripheral Tissues: A Focus on Butyrate, Colon Cancer, Obesity and Insulin Resistance. Nutrients. 2017;9(12). doi:10.3390/nu9121348
70. Ayd?n E, Türkez H, Kele? MS. Potential anticancer activity of carvone in N2a neuroblastoma cell line. Toxicol Ind Health. 2015;31(8):764-772. doi:10.1177/0748233713484660
71. Souza FVM, da Rocha MB, de Souza DP, Marçal RM. (?)-Carvone: Antispasmodic effect and mode of action. Fitoterapia. 2013;85:20-24. doi:10.1016/j.fitote.2012.10.012
72. Muruganathan U, Srinivasan S. Beneficial effect of carvone, a dietary monoterpene ameliorates hyperglycemia by regulating the key enzymes activities of carbohydrate metabolism in streptozotocin-induced diabetic rats. Biomed Pharmacother. 2016;84:1558-1567. doi:10.1016/j.biopha.2016.11.025
73. Nogoceke FP, Barcaro IMR, de Sousa DP, Andreatini R. Antimanic-like effects of (R)-(?)-carvone and (S)-(+)-carvone in mice. Neurosci Lett. 2016;619:43-48. doi:10.1016/j.neulet.2016.03.013
74. de Carvalho CCCR, da Fonseca MMR. Carvone: Why and how should one bother to produce this terpene. Food Chem. 2006;95(3):413-422. doi:10.1016/J.FOODCHEM.2005.01.003
75. Zhu R, Liu H, Liu C, et al. Cinnamaldehyde in diabetes: A review of pharmacology, pharmacokinetics and safety. Pharmacol Res. 2017;122:78-89. doi:10.1016/j.phrs.2017.05.019
76. Chen B-J, Fu C-S, Li G-H, et al. Cinnamaldehyde Analogues as Potential Therapeutic Agents. Mini Rev Med Chem. 2017;17(1):33-43. http://www.ncbi.nlm.nih.gov/pubmed/26791737. Accessed December 25, 2018.
77. Friedman M. Chemistry, Antimicrobial Mechanisms, and Antibiotic Activities of Cinnamaldehyde against Pathogenic Bacteria in Animal Feeds and Human Foods. J Agric Food Chem. 2017;65(48):10406-10423. doi:10.1021/acs.jafc.7b04344
78. Shreaz S, Wani WA, Behbehani JM, et al. Cinnamaldehyde and its derivatives, a novel class of antifungal agents. Fitoterapia. 2016;112:116-131. doi:10.1016/j.fitote.2016.05.016
79. Pérez Zamora C, Torres C, Nuñez M. Antimicrobial Activity and Chemical Composition of Essential Oils from Verbenaceae Species Growing in South America. Molecules. 2018;23(3):544. doi:10.3390/molecules23030544
80. Opinion of the Scientific Panel on Food Additives, Flavourings, Processing Aids and Materials in Contact with Food (AFC) on a Request from the Commission Related to Flavouring Group Evaluation 23: Aliphatic, Alicyclic and Aromatic Ethers Including Anisole Derivatives From Chemical Groups 15, 16 and 26 (Commission Regulation (EC) No.; 1565. http://www.efsa.europa.eu/sites/default/files/scientific_output/files/main_documents/417.pdf. Accessed December 25, 2018.
81. Patel S. Plant essential oils and allied volatile fractions as multifunctional additives in meat and fish-based food products: a review. Food Addit Contam Part A. 2015;32(7):1049-1064. doi:10.1080/19440049.2015.1040081
82. Liu K, Chen Q, Liu Y, Zhou X, Wang X. Isolation and Biological Activities of Decanal, Linalool, Valencene, and Octanal from Sweet Orange Oil. J Food Sci. 2012;77(11):C1156-C1161. doi:10.1111/j.1750-3841.2012.02924.x
83. Laribi B, Kouki K, M’Hamdi M, Bettaieb T. Coriander (Coriandrum sativum L.) and its bioactive constituents. Fitoterapia. 2015;103:9-26. doi:10.1016/j.fitote.2015.03.012
84. EFSA Panel on Additives and Products or Substances used in Animal Feed (FEEDAP). Scientific Opinion on the safety and efficacy of straight-chain primary aliphatic alcohols/aldehydes/acids, acetals and esters with esters containing saturated alcohols and acetals containing saturated aldehydes (chemical group 1) when used as flavourings. EFSA J. 2013;11(4):3169.
85. Chhikara N, Kour R, Jaglan S, Gupta P, Gat Y, Panghal A. Citrus medica: nutritional, phytochemical composition and health benefits – a review. Food Funct. 2018;9(4):1978-1992. doi:10.1039/c7fo02035j
86. Dunnington D, Butterworth KR, Gaunt IF, Mason PL, Evans JG, Gangolli SD. Long-term toxicity study of ethyl methylphenylglycidate (strawberry aldehyde) in the rat. Food Cosmet Toxicol. 1981;19:691-699. doi:10.1016/0015-6264(81)90522-8
87. Khalil AA, Rahman U ur, Khan MR, Sahar A, Mehmood T, Khan M. Essential oil eugenol: sources, extraction techniques and nutraceutical perspectives. RSC Adv. 2017;7(52):32669-32681. doi:10.1039/C7RA04803C
88. Flavouring Group Evaluation 60 (FGE.60) 1?: Consideration of Eugenol and Related Hydroxyallylbenzene Derivatives Evaluated by JECFA (65 Th Meeting) Structurally Related to Ring-Substituted Phenolic Substances Evaluated by EFSA in FGE.22 (2006) Opinion of the Scientific Panel on Food Additives, Flavourings, Processing Aids and Materials in Contact with Food (AFC). http://www.efsa.europa.eu/EFSA/efsa_locale-1178620753812_1178620772628.htm. Accessed December 25, 2018.
89. Hu Q, Zhou M, wei S. Progress on the Antimicrobial Activity Research of Clove Oil and Eugenol in the Food Antisepsis Field. J Food Sci. 2018;83(6):1476-1483. doi:10.1111/1750-3841.14180
90. Api AM, Belsito D, Bhatia S, et al. RIFM fragrance ingredient safety assessment, Eugenol, CAS Registry Number 97-53-0. Food Chem Toxicol. 2016;97:S25-S37. doi:10.1016/j.fct.2015.12.013
91. Marchese A, Barbieri R, Coppo E, et al. Antimicrobial activity of eugenol and essential oils containing eugenol: A mechanistic viewpoint. Crit Rev Microbiol. 2017;43(6):668-689. doi:10.1080/1040841X.2017.1295225
92. Fujisawa S, Murakami Y. Eugenol and Its Role in Chronic Diseases. In: Advances in Experimental Medicine and Biology. Vol 929. ; 2016:45-66. doi:10.1007/978-3-319-41342-6_3
93. Food and Drug Administration. CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=184.1257. Accessed December 25, 2018.
95. Seebaluck R, Gurib-Fakim A, Mahomoodally F. Medicinal plants from the genus Acalypha (Euphorbiaceae)–A review of their ethnopharmacology and phytochemistry. J Ethnopharmacol. 2015;159:137-157. doi:10.1016/j.jep.2014.10.040
96. Qi F, Yan Q, Zheng Z, Liu J, Chen Y, Zhang G. Geraniol and geranyl acetate induce potent anticancer effects in colon cancer Colo-205 cells by inducing apoptosis, DNA damage and cell cycle arrest. J BUON. 23(2):346-352. http://www.ncbi.nlm.nih.gov/pubmed/29745075. Accessed December 25, 2018.
97. National Toxicology Program. NTP Carcinogenesis Studies of Food Grade Geranyl Acetate (71% Geranyl Acetate, 29% Citronellyl Acetate) (CAS No. 105-87-3) in F344/N Rats and B6C3F1 Mice (Gavage Study). Natl Toxicol Program Tech Rep Ser. 1987;252:1-162. http://www.ncbi.nlm.nih.gov/pubmed/12748693. Accessed December 25, 2018.
98. Heidor R, Ortega JF, de Conti A, Ong TP, Moreno FS. Anticarcinogenic actions of tributyrin, a butyric acid prodrug. Curr Drug Targets. 2012;13(14):1720-1729. http://www.ncbi.nlm.nih.gov/pubmed/23140283. Accessed December 26, 2018.
99. Bedford A, Gong J. Implications of butyrate and its derivatives for gut health and animal production. Anim Nutr. 2018;4(2):151-159. doi:10.1016/J.ANINU.2017.08.010
100. Kuefer R, Hofer MD, Altug V, et al. Sodium butyrate and tributyrin induce in vivo growth inhibition and apoptosis in human prostate cancer. Br J Cancer. 2004;90(2):535-541. doi:10.1038/sj.bjc.6601510
101. Kang SN, Lee E, Lee M-K, Lim S-J. Preparation and evaluation of tributyrin emulsion as a potent anti-cancer agent against melanoma. Drug Deliv. 2011;18(2):143-149. doi:10.3109/10717544.2010.522610
102. Cresci GA, Glueck B, McMullen MR, Xin W, Allende D, Nagy LE. Prophylactic tributyrin treatment mitigates chronic-binge ethanol-induced intestinal barrier and liver injury. J Gastroenterol Hepatol. 2017;32(9):1587-1597. doi:10.1111/jgh.13731
103. Aquilina G, Bach A, Bampidis V, et al. Scientific Opinion on the safety and efficacy of branched-chain primary aliphatic alcohols/aldehydes/acids, acetals and esters with esters containing branched-chain alcohols and acetals containing branched-chain aldehydes (chemical group 2) when used as flavourings for all animal species 1 EFSA Panel on Additives and Products or Substances used in Animal Feed (FEEDAP). EFSA J. 2012;10(10):2927. doi:10.2903/j.efsa.2012.2927
104. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21. 21CFR184.1903; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=184.1903. Accessed December 26, 2018.
105. Sun J. D-Limonene: safety and clinical applications. Altern Med Rev. 2007;12(3):259-264. http://www.ncbi.nlm.nih.gov/pubmed/18072821. Accessed December 26, 2018.
106. Vieira AJ, Beserra FP, Souza MC, Totti BM, Rozza AL. Limonene: Aroma of innovation in health and disease. Chem Biol Interact. 2018;283:97-106. doi:10.1016/j.cbi.2018.02.007
107. Ravichandran C, Badgujar PC, Gundev P, Upadhyay A. Review of toxicological assessment of d-limonene, a food and cosmetics additive. Food Chem Toxicol. 2018;120:668-680. doi:10.1016/j.fct.2018.07.052
108. Kim YW, Kim MJ, Chung BY, et al. Safety evaluation and risk assessment of D-limonene. J Toxicol Environ Heal – Part B Crit Rev. 2013;16(1):17-38. doi:10.1080/10937404.2013.769418
109. Scientific Opinion on the safety and efficacy of aliphatic and aromatic hydrocarbons (chemical group 31) when used as flavourings for all animal species; Scientific Opinion on the safety and efficacy of aliphatic and aromatic hydrocarbons (chemical group 31) when used as flavourings for all animal species. EFSA J. 2015;13(3):4053. doi:10.2903/j.efsa.2015.4053
110. Pereira I, Severino P, Santos AC, Silva AM, Souto EB. Linalool bioactive properties and potential applicability in drug delivery systems. Colloids Surfaces B Biointerfaces. 2018;171:566-578. doi:10.1016/j.colsurfb.2018.08.001
111. Seol G-H, Kang P, Lee HS, Seol GH. Antioxidant activity of linalool in patients with carpal tunnel syndrome. BMC Neurol. 2016;16(1):17. doi:10.1186/s12883-016-0541-3
112. de Oliveira Lima MI, Araújo de Medeiros AC, Souza Silva KV, Cardoso GN, de Oliveira Lima E, de Oliveira Pereira F. Investigation of the antifungal potential of linalool against clinical isolates of fluconazole resistant Trichophyton rubrum. J Mycol Med. 2017;27(2):195-202. doi:10.1016/j.mycmed.2017.01.011
113. Iwasaki K, Zheng Y-W, Murata S, et al. Anticancer effect of linalool viacancer-specific hydroxyl radical generation in human colon cancer. World J Gastroenterol. 2016;22(44):9765. doi:10.3748/wjg.v22.i44.9765
114. Herman A, Tambor K, Herman A. Linalool Affects the Antimicrobial Efficacy of Essential Oils. Curr Microbiol. 2016;72(2):165-172. doi:10.1007/s00284-015-0933-4
115. Scientific Opinion on the safety and efficacy of aliphatic, alicyclic and aromatic saturated and unsaturated tertiary alcohols and esters with esters containing tertiary alcohols ethers (chemical group 6) when used as flavourings for all animal species. EFSA J. 2012;10(11):2966. doi:10.2903/j.efsa.2012.2966
116. Rombolà L, Amantea D, Russo R, et al. Rational Basis for the Use of Bergamot Essential Oil in Complementary Medicine to Treat Chronic Pain. Mini Rev Med Chem. 2016;16(9):721-728. http://www.ncbi.nlm.nih.gov/pubmed/26996621. Accessed December 26, 2018.
117. Koulivand PH, Khaleghi Ghadiri M, Gorji A. Lavender and the nervous system. Evid Based Complement Alternat Med. 2013;2013:681304. doi:10.1155/2013/681304
118. National Center for Biotechnology Information. Malic Acid. PubChem Compound Database.
119. Abraham GE, Flechas JD. Management of Fibromyalgia: Rationale for the Use of Magnesium and Malic Acid. J Nutr Med. 1992;3(1):49-59. doi:10.3109/13590849208997961
120. Tyka AK, Chwastowski M, Cison T, et al. Effect of creatine malate supplementation on physical performance, body composition and selected hormone levels in spinters and long-distance runners. Acta Physiol Hung. 2015;102(1):114-122. doi:10.1556/APhysiol.102.2015.1.12
121. Rodgers AL, Webber D, de Charmoy R, Jackson GE, Ravenscroft N. Malic Acid Supplementation Increases Urinary Citrate Excretion and Urinary pH: Implications for the Potential Treatment of Calcium Oxalate Stone Disease. J Endourol. 2014;28(2):229-236. doi:10.1089/end.2013.0477
122. National Center for Biotechnology Information. Methyl Anthranilate. PubChem Database.
123. Askham LR. Proceedings – Vertebrate Pest Conference. In: Proceedings… Vertebrate Pest Conference (USA). University of California, Davis; 1992. http://agris.fao.org/agris-search/search.do?recordID=US9416552. Accessed December 26, 2018.
124. Cummings JL, Avery ML, Pochop PA, et al. Evaluation of a methyl anthranilate formulation for reducing bird damage to blueberries. Crop Prot. 1995;14(3):257-259. doi:10.1016/0261-2194(95)00016-F
125. Aquilina G, Bories G, Chesson A, et al. Scientific Opinion on the safety and efficacy of anthranilate derivatives (chemical group 27) when used as flavourings for all animal species 1 EFSA Panel on Additives and Products or Substances used in Animal Feed (FEEDAP) Anthranilate derivatives (CG 27) for all species. EFSA J. 2011;9(12):2441. doi:10.2903/j.efsa.2011.2441
126. Rao VRS, Raju SS, Sarma VU, et al. Simultaneous determination of bioactive compounds in Piper nigrum L. and a species comparison study using HPLC-PDA. Nat Prod Res. 2011;25(13):1288-1294. doi:10.1080/14786419.2010.535158
127. Li X, Choi Y, Yanakawa Y, Park T. Piperonal prevents high-fat diet-induced hepatic steatosis and insulin resistance in mice via activation of adiponectin/AMPK pathway. Int J Obes. 2014;38(1):140-147. doi:10.1038/ijo.2013.70
128. Chu S, Narayan VP, Sung M-K, Park T. Piperonal attenuates visceral adiposity in mice fed a high-fat diet: potential involvement of the adenylate cyclase-protein kinase A dependent pathway. Mol Nutr Food Res. 2017;61(11):1601124. doi:10.1002/mnfr.201601124
129. Meriga B, Parim B, Chunduri VR, et al. Antiobesity potential of Piperonal: promising modulation of body composition, lipid profiles and obesogenic marker expression in HFD-induced obese rats. Nutr Metab (Lond). 2017;14(1):72. doi:10.1186/s12986-017-0228-9
130. Anantharaju PG, Gowda PC, Vimalambike MG, Madhunapantula S V. An overview on the role of dietary phenolics for the treatment of cancers. Nutr J. 2016;15(1):99. doi:10.1186/s12937-016-0217-2
131. del Olmo A, Calzada J, Nuñez M. Benzoic acid and its derivatives as naturally occurring compounds in foods and as additives: Uses, exposure, and controversy. Crit Rev Food Sci Nutr. 2017;57(14):3084-3103. doi:10.1080/10408398.2015.1087964
132. Aguilar F, Crebelli R, Domenico A Di, et al. Scientific Opinion on the re-evaluation of benzoic acid (E 210), sodium benzoate (E 211), potassium benzoate (E 212) and calcium benzoate (E 213) as food additives; Scientific Opinion on the re-evaluation of benzoic acid (E 210), sodium benzoate (E 211), potassium benzoate (E 212) and calcium benzoate (E 213) as food additives. EFSA J. 2016;14(3):110. doi:10.2903/j.efsa.2016.4433
133. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=184.1021. Accessed December 26, 2018.
134. Qualley A V., Widhalm JR, Adebesin F, Kish CM, Dudareva N. Completion of the core -oxidative pathway of benzoic acid biosynthesis in plants. Proc Natl Acad Sci. 2012;109(40):16383-16388. doi:10.1073/pnas.1211001109
135. Andersen FA. Final report on the safety assessment of Benzyl Alcohol, Benzoic Acid, and Sodium Benzoate. In:International Journal of Toxicology. Vol 20. ; 2001:23-50. doi:10.1080/10915810152630729
136. Food Standards Authority Australia New Zealand (FSANZ). SCHEDULE 1 Permitted Uses of Food Additives by Food Type. http://www.foodstandards.gov.au/code/Documents/standard_1_3_1_additives_vol_2_v1321.pdf. Accessed December 27, 2018.
137. Fidler MC, Davidsson L, Zeder C, Hurrell RF. Erythorbic acid is a potent enhancer of nonheme-iron absorption.Am J Clin Nutr. 2004;79(1):99-102. doi:10.1093/ajcn/79.1.99
138. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=182.3041. Accessed December 27, 2018.
139. Aguilar F, Crebelli R, Domenico A Di, et al. Scientific Opinion on the re-evaluation of erythorbic acid (E 315) and sodium erythorbate (E 316) as food additives; Scientific Opinion on the re-evaluation of erythorbic acid (E 315) and sodium erythorbate (E 316) as food additives. EFSA J. 2016;14(1):4360-4362. doi:10.2903/j.efsa.2016.4360
140. Miura K, Yazama F, Tai A. Oxidative stress-mediated antitumor activity of erythorbic acid in high doses. Biochem Biophys Reports. 2015;3:117-122. doi:10.1016/j.bbrep.2015.07.018
141. Scientific Opinion on the safety evaluation of the substance, thiodipropionic acid, ditetradecyl ester, CAS No. 16545-54-3, for use in food contact materials. EFSA J. 2011;9(4):2126. doi:10.2903/j.efsa.2011.2126
142. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=182.3109. Accessed December 27, 2018.
143. Hocman G. Chemoprevention of cancer: phenolic antioxidants (BHT, BHA). Int J Biochem. 1988;20(7):639-651. http://www.ncbi.nlm.nih.gov/pubmed/3053283. Accessed December 27, 2018.
144. Laflamme D, Izquierdo O, Eirmann L, Binder S. Myths and Misperceptions About Ingredients Used in Commercial Pet Foods. Vet Clin North Am Small Anim Pract. 2014;44(4):689-698. doi:10.1016/j.cvsm.2014.03.002
145. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfCFR/CFRSearch.cfm?fr=182.3169. Accessed December 27, 2018.
146. Rychen G, Aquilina G, Azimonti G, et al. Safety and efficacy of butylated hydroxyanisole (BHA) as a feed additive for all animal species. EFSA J. 2018;16(3). doi:10.2903/j.efsa.2018.5215
147. Iverson F. Phenolic antioxidants: Health protection branch studies on butylated hydroxyanisole. Cancer Lett. 1995;93(1):49-54. doi:10.1016/0304-3835(95)03787-W
148. Kahl R, Kappus H. [Toxicology of the synthetic antioxidants BHA and BHT in comparison with the natural antioxidant vitamin E]. Z Lebensm Unters Forsch. 1993;196(4):329-338. http://www.ncbi.nlm.nih.gov/pubmed/8493816. Accessed December 27, 2018.
149. Williams GM, Iatropoulos MJ, Whysner J. Safety assessment of butylated hydroxyanisole and butylated hydroxytoluene as antioxidant food additives. Food Chem Toxicol. 37(9-10):1027-1038. http://www.ncbi.nlm.nih.gov/pubmed/10541460. Accessed December 27, 2018.
150. Hirose M, Yada H, Hakoi K, Takahashi S, Ito N. Modification of carcinogenesis by alpha-tocopherol, t-butylhydroquinone, propyl gallate and butylated hydroxytoluene in a rat multi-organ carcinogenesis model. Carcinogenesis. 1993;14(11):2359-2364. http://www.ncbi.nlm.nih.gov/pubmed/8242867. Accessed December 27, 2018.
151. Aguilar R, Crebelli B, Dusemund P, et al. EFSA Panel on Food Additives and Nutrient Sources added to Food (ANS); Scientific Opinion on the re-evaluation of Butylated hydroxytoluene BHT (E 321) as a food additive Scientific Opinion on the re-evaluation of butylated hydroxytoluene BHT (E 321) as a . EFSA J. 2012;10(3):2588-2590. doi:10.2903/j.efsa.2012.2588
152. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=182.3225. Accessed December 27, 2018.
153. Dzanis DA. Safety of Ethoxyquin in Dog Foods. J Nutr. 1991;121(suppl_11):S163-S164. doi:10.1093/jn/121.suppl_11.S163
154. CABEL MC, WALDROUP PW, SHERMER WD, CALABOTTA DF. Effects of Ethoxyquin Feed Preservative and Peroxide Level on Broiler Performance. Poult Sci. 1988;67(12):1725-1730. doi:10.3382/ps.0671725
155. Zhu J, Carozzi VA, Reed N, et al. Ethoxyquin provides neuroprotection against cisplatin-induced neurotoxicity. Sci Rep. 2016;6(1):28861. doi:10.1038/srep28861
156. Safety and efficacy of ethoxyquin (6?ethoxy?1,2?dihydro?2,2,4?trimethylquinoline) for all animal species. EFSA J. 2015;13(11). doi:10.2903/j.efsa.2015.4272
157. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=573.380. Accessed December 27, 2018.
158. Zhu J, Chen W, Mi R, Zhou C, Reed N, Höke A. Ethoxyquin prevents chemotherapy-induced neurotoxicity via Hsp90 modulation. Ann Neurol. 2013;74(6):893-904. doi:10.1002/ana.24004
159. B?aszczyk A, Augustyniak A, Skolimowski J. Ethoxyquin: An Antioxidant Used in Animal Feed. Int J Food Sci. 2013;2013:1-12. doi:10.1155/2013/585931
160. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=182.3280&SearchTerm=dilauryl thiodipropionate. Accessed December 27, 2018.
161. Sasseville D, Alfalah M, Lacroix J-P. “Parabenoia” Debunked, or “Who’s Afraid of Parabens?”. Dermatitis. 2015;26(6):254-259. doi:10.1097/DER.0000000000000147
162. Soni MG, Taylor SL, Greenberg NA, Burdock GA. Evaluation of the health aspects of methyl paraben: a review of the published literature. Food Chem Toxicol. 2002;40(10):1335-1373. http://www.ncbi.nlm.nih.gov/pubmed/12387298. Accessed December 27, 2018.
163. Opinion of the Scientific Panel on Food Additives, Flavourings, Processing Aids and Materials in Contact with Food on a Request from the Commission Related to Para Hydroxybenzoates The Scientific Panel on Food Additives, Flavourings, Processing Aids and Materials In.; 2004. http://www.efsa.europa.eu/sites/default/files/scientific_output/files/main_documents/83.pdf. Accessed December 27, 2018.
164. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=184.1670. Accessed December 27, 2018.
165. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=184.1490&SearchTerm=methylparaben . Accessed December 27, 2018.
166. Scientific Opinion on the re?evaluation of sulfur dioxide (E 220), sodium sulfite (E 221), sodium bisulfite (E 222), sodium metabisulfite (E 223), potassium metabisulfite (E 224), calcium sulfite (E 226), calcium bisulfite (E 227) and potassium bisulfite (E 228) as food additives. EFSA J. 2016;14(4). doi:10.2903/j.efsa.2016.4438
167. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=182.3637. Accessed December 27, 2018.
168. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=182.3616. Accessed December 27, 2018.
169. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=182.3766. Accessed December 27, 2018.
170. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=182.3798. Accessed December 27, 2018.
171. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=182.3739. Accessed December 27, 2018.
172. Beckman Sundh U, Binderup M-L, Bolognesi C, et al. Scientific Opinion on the safety evaluation… CEF); Sci EFSA J. 2013;11(4):3155. doi:10.2903/j.efsa.2013.3155
173. Zar T, Graeber C, Perazella MA. Reviews: Recognition, Treatment, and Prevention of Propylene Glycol Toxicity. Semin Dial. 2007;20(3):217-219. doi:10.1111/j.1525-139X.2007.00280.x
174. Tobe M, Furuya T, Kawasaki Y, et al. Six-month toxicity study of butylated hydroxyanisole in beagle dogs. Food Chem Toxicol. 24(10-11):1223-1228. http://www.ncbi.nlm.nih.gov/pubmed/3804124. Accessed December 27, 2018.
175. Weil CS, Woodside MD, Smyth HF, Carpenter CP. Results of feeding propylene glycol in the diet to dogs for two years. Food Cosmet Toxicol. 1971;9(4):479-490. doi:10.1016/0015-6264(71)90078-2
176. Agency for Toxic Substances and Disease Registry, Public Health Service USD of H and HS. TOXICOLOGICAL PROFILE FOR PROPYLENE GLYCOL. Atlanta, GA; 1997. https://www.atsdr.cdc.gov/toxprofiles/tp189.pdf. Accessed December 27, 2018.
177. Staples CA, Davis JW. An examination of the physical properties, fate, ecotoxicity and potential environmental risks for a series of propylene glycol ethers. Chemosphere. 2002;49(1):61-73. http://www.ncbi.nlm.nih.gov/pubmed/12243331. Accessed December 27, 2018.
178. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/cfrsearch.cfm?fr=184.1666. Accessed December 27, 2018.
179. Bigner DR, Goff JP, Faust MA, Tyler HD, Horst RL. Comparison of Oral Sodium Compounds for the Correction of Acidosis. J Dairy Sci. 1997;80(9):2162-2166. doi:10.3168/jds.S0022-0302(97)76163-0
180. SCHULTZ LH. Treatment of ketosis in dairy cattle with sodium propionate. Cornell Vet. 1952;42(1):148-155. http://www.ncbi.nlm.nih.gov/pubmed/14905895. Accessed December 27, 2018.
181. Kishimoto Y, Wakabayashi S, Takeda H. Effects of intravenous injection and intraperitoneal continual administration of sodium propionate on serum cholesterol levels in rats. J Nutr Sci Vitaminol (Tokyo). 1995;41(1):73-81. http://www.ncbi.nlm.nih.gov/pubmed/7616328. Accessed December 27, 2018.
182. Wang J, Wei Z, Zhang X, Wang Y, Yang Z, Fu Y. Propionate Protects against Lipopolysaccharide-Induced Mastitis in Mice by Restoring Blood–Milk Barrier Disruption and Suppressing Inflammatory Response. Front Immunol. 2017;8. doi:10.3389/fimmu.2017.01108
183. Chambers ES, Byrne CS, Aspey K, et al. Acute oral sodium propionate supplementation raises resting energy expenditure and lipid oxidation in fasted humans. Diabetes, Obes Metab. 2018;20(4):1034-1039. doi:10.1111/dom.13159
184. Safari R, Hoseinifar SH, Kavandi M. Modulation of antioxidant defense and immune response in zebra fish (Danio rerio) using dietary sodium propionate. Fish Physiol Biochem. 2016;42(6):1733-1739. doi:10.1007/s10695-016-0253-z
185. Safety of the extension of use of sodium propionate (E 281) as a food additive. EFSA J. 2016;14(8). doi:10.2903/j.efsa.2016.4546
186. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=184.1784. Accessed December 27, 2018.
187. Silva De Souza SM, Hirata R, Moreira LO, et al. Influence of stannous chloride on the adhesive properties of Corynebacterium diphtheriae strains. Int J Mol Med. 2003;12(4):657-661. http://www.ncbi.nlm.nih.gov/pubmed/12964050. Accessed December 27, 2018.
188. João-Souza SH, Bezerra SJC, de Freitas PM, et al. In situ evaluation of fluoride-, stannous- and polyphosphate-containing solutions against enamel erosion. J Dent. 2017;63:30-35. doi:10.1016/j.jdent.2017.05.014
189. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=184.1845. Accessed December 27, 2018.
190. Younes M, Aggett P, Aguilar F, et al. Re?evaluation of stannous chloride (E 512) as food additive. EFSA J. 2018;16(6). doi:10.2903/j.efsa.2018.5295
191. Wang X-B, Cui H, Liu X, Du J-B. Sulfur dioxide: foe or friend for life? Histol Histopathol. 2017;32(12):1231-1238. doi:10.14670/HH-11-904
192. Oehha. Sulfur Dioxide in Dried Fruit, Interpretive Guidelines.; 2012. http://www.oehha.ca.gov/prop65/prop65_list/Newlist.html. Accessed December 27, 2018.
193. Freedman BJ. Sulphur dioxide in foods and beverages: its use as a preservative and its effect on asthma. Br J Dis Chest. 1980;74(2):128-134. http://www.ncbi.nlm.nih.gov/pubmed/7426352. Accessed December 27, 2018.
194. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=182.3862. Accessed December 27, 2018.
195. Chen S, Zheng S, Liu Z, et al. Endogeous sulfur dioxide protects against oleic acid-induced acute lung injury in association with inhibition of oxidative stress in rats. Lab Investig. 2015;95(2):142-156. doi:10.1038/labinvest.2014.147
196. Wang L-F, Su S-W, Wang L, et al. Tert-butylhydroquinone ameliorates doxorubicin-induced cardiotoxicity by activating Nrf2 and inducing the expression of its target genes. Am J Transl Res. 2015;7(10):1724-1735. http://www.ncbi.nlm.nih.gov/pubmed/26692920. Accessed December 27, 2018.
197. Zeng X-P, Li X-J, Zhang Q-Y, et al. Tert-Butylhydroquinone Protects Liver Against Ischemia/Reperfusion Injury in Rats Through Nrf2-Activating Anti-Oxidative Activity. Transplant Proc. 2017;49(2):366-372. doi:10.1016/j.transproceed.2016.12.008
198. Zhou N-Q, Liu N, Li P, Ping S, Peng Q-S, Shi W-D. Tert-butylhydroquinone promotes angiogenesis and improves heart functions in rats after myocardial infarction. Clin Exp Hypertens. 2017;39(5):402-408. doi:10.1080/10641963.2016.1259322
199. Gharavi N, Haggarty S, El-Kadi AOS. Chemoprotective and carcinogenic effects of tert-butylhydroquinone and its metabolites. Curr Drug Metab. 2007;8(1):1-7. http://www.ncbi.nlm.nih.gov/pubmed/17266519. Accessed December 27, 2018.
200. van Esch GJ. Toxicology of tert-butylhydroquinone (TBHQ). Food Chem Toxicol. 1986;24(10-11):1063-1065. doi:10.1016/0278-6915(86)90289-9
201. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=172.185. Accessed December 27, 2018.
202. Opinion of the Scientific Panel on food additives, flavourings, processing aids and materials in contact with food (AFC) on a request from the Commission related to tertiary-Butylhydroquinone (TBHQ). EFSA J. 2004;2(10):84. doi:10.2903/j.efsa.2004.84
203. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfCFR/CFRSearch.cfm?fr=74.250. Accessed December 25, 2018.
204. Food and Drug Administration (FDA). CFR – Code of Federal Regulations Title 21.; 2018. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfCFR/CFRSearch.cfm?fr=74.302. Accessed December 25, 2018.
In 2017 and 2018, I covered extensivelythe efforts of the American College of Veterinary Botanical Medicine (ACVBM) to achieve recognition as a medical specialty by the American Board of Veterinary Specialties (ABVS). I opposed recognition for several reasons:
Prescribing of herbal medicine in the veterinary field is based mostly on folk medicine traditions, especially Traditional Chinese Veterinary Medicine (TCVM), which are mostly unproven and often deeply inconsistent with scientific medicine.
Most herbalists, including leaders of the ACVBM, promote many alternative therapies other than herbal medicine, and these people often have medical philosophies inconsistent with science and science-based medicine.
Very few herbal remedies have been properly tested scientifically, so there is an insufficient foundation of knowledge to justify a specialty. What scientific work has been done in this area falls naturally under the domain of existing specialty organizations, such as the American College of Veterinary Clinical Pharmacology (ACVCP), so there is no need to create a new college.
Herbalism is not a recognized medical specialty in human or veterinary medicine in Europe, Australia, or the United States because it has not yet developed a legitimate scientific basis, and recognition of the ACVBM would give a misleading appearance of scientific legitimacy to a set of approaches reliant predominantly on folk traditions.
The ABVS tabled the ACVBM petitionand recommended the group seek subspecialty status under the ACVCP. The ABVS process is quite secretive, so little has been made public about it, but it appears that ACVCP wished to set up a methodical and careful process to consider any potential relationship between the groups, and the ACVBM decided it did not wish to pursue this process. Instead, the ACVBM has reactivated the tabled application for standalone recognition from ABVS. The latest version of the ACVBM petitiondiffers in some respects from the original petition submitted in 2016. The original petition, and subsequent communications with ABVS, tried to emphasize the mainstream, scientific nature of herbal medicine and downplay the alternative nature of the practice. The current petition does this as well, but it seems to emphasize more strongly the differences between a science-based approach to medicine and the philosophy of herbalism derived from traditional sources.
Here are a few examples:
Botanical medicine looks at pharmacognosy, not from the perspective of single molecule phytochemical discovery for the development of new drug leads, but rather to validate or understand traditional medicine and how the herbs work….That the whole plant is more therapeutic than a constituent is a fundamental principle of botanical medicine supported by research.
Principles of botanical medicine respect tradition as a source of empirical evidence that informs formal research design. The study of traditional use of plants within a culture is termed ethnobotany, and the study of traditional medicines is known as ethnomedicine, or ethnoveterinary medicine. Research may validate traditional uses.
Research may validate traditional use, or it may not (which is more common but not acknowledged in the petition). This statement clearly shows the unscientific view that the goal of research is to “validate or understand” the beliefs of traditional folk medicine, rather than to test them and find out if they are true or not. It also accepts as a central principle the traditional notion that whole plants are more effective than isolated plant compounds, though there is virtually no real-world research evidence supporting this idea.
The ACVBM differentiates themselves by interest in the rich knowledge base of traditional botanical medicine use and ethnobotany combined with modern scientific, chemical, toxicological, pharmacological clinical application and research in a practice that could be appropriately termed rationale phytotherapy to distinguish from colleagues who may only embrace traditional findings or who may eschew scientific findings…
This is encouraging, though given the background and other practices of the organizing committee for the ACVBM, I am not convince that the organization is likely to ever give priority to science over traditional knowledge if the two conflict. TCVM vets and practitioners of homeopathy and not really the most reliable guardians of science-based practice.
Veterinarians using botanical medicine have a patient centered approach, whereby the botanical medicines are selected based on the individual signs and pathophysiology as well as the diagnosis. So that two dogs with diabetes for example, may be treated with two different sets of botanical medicines.
This is the common claim of alternative medicine to “individualize” therapy to a greater extent than scientific medicine. I’ve written many times beforeabout why this is a misleading and empty claim that hides the fact that such supposedly “individualized” therapies are almost never scientifically tested or shown to be effective or superior in any way to science-based practices.
The ACVBM also holds the philosophical position, common in alternative medicine, that tradition and personal or anecdotal experience are reliable and sufficient evidence and may even be superior to controlled scientific research. Here are some illustrations:
Sources of information include:
Traditional use. The bewildering variety of ethnoveterinary practices, ethnobotanical uses and folk practices around the world coupled with confounding aspects of cultural, placebo and other non-specific effects make reliable conclusions from any one tradition difficult. Frequently however, traditional use informs research and pharmacological activity is often found to be closely correlated. There are recurring themes in traditional medicine and persistent therapeutic approaches consistent with the use of “archetypal” chemical groups within plants.
I certainly agree that traditional use is inconsistent, low-quality evidence that has rarely led to definitive success in treatment. I disagree, however, with the claim that scientific evidence frequently confirms traditional use. Folk herbalism often uses plants for a wide variety of unrelated problems, and when properly tested the rare few uses which seem to have some real benefits are celebrated and the many that were useless are forgotten.
Collective clinical experience over decades. There is also the clinical experience of veterinary practitioners to consider- thousands of educated veterinary practitioners worldwide prescribe herbal medicines in their work. This has advantages of being in a modern veterinary context. Veterinary practitioners of botanical medicine have written texts and taught other veterinarians to achieve repeatable results within the botanical framework.
Collective clinical experience is another way of saying “anecdote,” and as the saying goes, the plural of “anecdote” is not “data.” The fact that people are “experts” in herbal medicine and have written and taught about it doesn’t, in itself, show that the beliefs and practices being passed along are correct or useful.
The third data source is substantial and scientifically sound but maybe not as clinically relevant to veterinary botanical medicine. The available published literature on phytochemistry and preclinical pharmacology…[this does] not however provide confirmation of a clinical effect; experience in practice is that the effect of the whole plant is rarely predicated on the effects of its parts….it is appreciated that herbs have been dismissed by many in the profession as the refuge of the uncritical. However, when all the sources of information come together and are integrated with pharmacological insights, something important happens; unique treatment strategies for treating notoriously difficult clinical problems become possible and the desire of the ACVBM is for animals to benefit from the efforts of this group to further develop the field. To be a fully effective therapy, it is not enough simply to know about the herbs themselves. Information must also be sought about how and when to use these herbs in response to various therapeutic challenges. Therapeutic approaches are different from those that underpin conventional medicine.
Again, this is a position that says scientific study, including pharmacological analysis of the compound sin plant remedies, is useful, but only as a supplement to the wisdom of tradition and personal experience, which still maintains without much evidence that traditional whole-plant remedies work better than plant-derived medicines. This is a pretty direct refutation of the principles of pharmacognosy (development of medicines from plants), which I suspect is a response to the rejection of the ACVBM by the ACVCP.
The universal role of plants in the treatment of disease is exemplified by their use in all the major systems of traditional medicine and ethnomedicine irrespective of their underlying philosophical premise.
So because lots of people have done it, this means it is worth doing? Not a rational perspective.
The practitioner of botanical medicine regards the whole formula or whole extract as the “active ” component” in the therapeutic context.
The concept of polyvalent or multifaceted activity of the medicine is central to botanical medicine – in the context of the advantage of chemical complexity -and even a single herbal extract is a natural multi agent medicine that can simultaneously target a range of desirable pharmacological effects.
The veterinary botanical practitioner prefers not just to prescribe chemically complex herbs, but often administers them in complex formulations, compared to conventional medicine preferring to prescribe a single drug. The practitioner chooses herbs or formulas for a cooperative or facilitating effect between the components to address therapeutic goals.
Again, these are tenets of faith, not scientifically proven propositions.
Philosophically the veterinary botanical medicine practitioner practices conventional medicine but overlays that practice with the use of botanical medicines in a framework of botanical principles to expand their options for treatment of disease and optimizing health.
Practitioners appreciate traditional knowledge as just one potential source of information, when coupled with published research and clinical experience, herbs can be prescribed safely and effectively.
This is the principle of “integrative medicine,” which holds that mixing the scientific with the unscientific and the proven with the unproven somehow makes the whole treatment approach better. As infectious disease doc Marc Crislip has put it, “If you integrate fantasy with reality, you do not instantiate reality. If you mix cow pie with apple pie, it does not make the cow pie taste better; it makes the apple pie worse.”
The ACVBM petition goes on to acknowledge that many veterinarians are concerned about the paucity of scientific research evidence concerning herbal medicine (though not to acknowledge directly that this is a well-founded concern). However, it then employs the tu quoquefallacy, arguing that since veterinary medicine as a whole suffers from a deficiency of high-quality research evidence, this should not be a barrier to treating herbal medicine as a legitimate scientific specialty. This misses the point, which is that we should be seeking more and better evidence, not giving up on the centrality of scientific research evidence to good medical practice. Giving the specialty imprimatur to an especially evidence-poor alternative practice only weakens the overall scientific basis of veterinary medicine.
An important basis of herbal medicine is the pharmacology and mechanisms of actions of plants and plant extracts, however they differ from drugs in their complexity, and in the underlying ethnomedical knowledge base used to initiate study of them. The botanical medicine diplomate can provide context to client and referring veterinarian inquiries, from both the ethnomedical and pharmacologic perspectives.
This basically suggests that the main reason herbalists should be considered specialists is that they can add the value of traditional knowledge to the scientific perspective on plant compounds. Again, this only makes sense if you presume, generally wrongly, that such traditional knowledge is useful or accurate much of the time.
Bottom Line
Nothing appears to have fundamentally changed in the ACVBM approach since I began to examine it in 2017. The ACVBM is a bit more direct in the latest petition in their claims that the primary reason they should be a distinct specialty group is because of their greater familiarity with traditional sources of knowledge about plant medicines. While they may acknowledge some need for scientific research into herbal remedies, they consistently claim that conventional veterinarians cannot effectively conduct such research without being familiar with the folk medicine approach to herbalism.
This implies that scientists cannot test the effectiveness of any medical therapy without being experts in prescientific folk beliefs about it. Can we not evaluate surgery without being experts in bloodletting? Is the study of antibiotics to treat syphilis futile unless we have first-hand training in the use of the poison mercury for treating this disease?
Ultimately, the ACVBM petition is simply another of the many efforts of alternative medicine to create an exception to the normal, scientific standards of evidence currently applied to medical practices. If scientific research works better than tradition or personal experience to determine which therapies are effective and why (and the evidence it does is overwhelming), then there is no need to give experts in folk medicine beliefs special status as experts in a discipline that can be readily and effectively studied with current scientific methods.
I believe there is great potential for effective medical therapies in plant chemistry, and we have already realized this in many modern drugs. I also believe folk tradition has only very rarely stumbled across truly effective treatments through trial-and-error and anecdote, and it is not a particularly useful guide to which plants we should study for which problems. Those herbalists truly committed to a scientific medical practice should work within the accepted standards of scientific evidence to validate (or invalidate) specific herbal practices, rather than trying to create a group that will exist primarily to promote and self-validate their own alternative standards of evidence.
A reader recently sent me a link to this little advertisement.
This is an illustration of a popular bit of alternative nonsense, the idea that raw milk has magical health-giving properties. The idea owes a lot to the Appeal to Nature Fallacy, the idea that something “natural” is inherently. Safer and healthier than something “artificial.” Of course, those words have little real meaning since the distinction is arbitrary and unreliable. And in any case, the effects of such “natural” substances as Salmonella, Ebola, Uranium, asbestos, and many others make it pretty obvious that natural does not mean safe or health.
Like so many proponents of irrational nutritional ideas, raw milk promoters exaggerate, ignore, and misuse science to create the illusion that there is real evidence behind their claims. They also make free use of anecdotes which, as I have discussed many times, prove absolutely nothing. The reality is that there is no reliable evidence that raw milk, from goats or any other species, has health benefits that can’t be obtained much more safely from pasteurized milk (that is, milk that has been heated to kill bacteria, parasites, and other dangerous microorganisms).
Many infants are exclusively fed unmodified goat’s milk as a result of cultural beliefs as well as exposure to false online information. Anecdotal reports have described a host of morbidities associated with that practice, including severe electrolyte abnormalities, metabolic acidosis, megaloblastic anemia, allergic reactions including life-threatening anaphylactic shock, hemolytic uremic syndrome, and infections. We describe here an infant who was fed raw goat’s milk and sustained intracranial infarctions in the setting of severe azotemia and hypernatremia, and we provide a comprehensive review of the consequences associated with this dangerous practice.
An increasing number of people are consuming raw unpasteurized milk. Enhanced nutritional qualities, taste, and health benefits have all been advocated as reasons for increased interest in raw milk consumption. However, science-based data to substantiate these claims are limited. People continue to consume raw milk even though numerous epidemiological studies have shown clearly that rawmilk can be contaminated by a variety of pathogens, some of which are associated with human illness and disease. Several documented milkborne disease outbreaks occurred from 2000-2008 and were traced back to consumption of raw unpasteurized milk. Numerous people were found to have infections, some were hospitalized, and a few died. In the majority of these outbreaks, the organism associated with the milkborne outbreak was isolated from the implicated product(s) or from subsequent products made at the suspected dairy or source. In contrast, fewer milkborne disease outbreaks were associated with consumption of pasteurized milk during this same time period. Twenty nine states allow the sale of raw milk by some means. Direct purchase, cow-share or leasing programs, and the sale of raw milk as pet food have been used as means for consumers to obtain raw milk. Where raw milk is offered for sale, strategies to reduce risks associated with raw milk and products made from raw milk are needed. Developing uniform regulations including microbial standards for raw milk to be sold for human consumption, labeling of raw milk, improving sanitation during milking, and enhancing and targeting educational efforts are potential approaches to this issue. Development of pre- and postharvest control measures to effectively reduce contamination is critical to the control of pathogens in raw milk. One sure way to prevent raw milk-associated foodborne illness is for consumers to refrain from drinking raw milk and from consuming dairy products manufactured using raw milk.
Sales of raw or unpasteurized milk and milk products are still legal in at least 30 states in the United States. Raw milk and milk products from cows, goats, and sheep continue to be a source of bacterial infections attributable to a number of virulent pathogens, including Listeria monocytogenes, Campylobacter jejuni, Salmonella species, Brucella species, and Escherichia coli O157. These infections can occur in both healthy and immunocompromised individuals, including older adults, infants, young children, and pregnant women and their unborn fetuses, in whom life-threatening infections and fetal miscarriage can occur. Efforts to limit the sale of raw milk products have met with opposition from those who are proponents of the purported health benefits of consuming raw milk products, which contain natural or unprocessed factors not inactivated by pasteurization. However, the benefits of these natural factors have not been clearly demonstrated in evidence-based studies and, therefore, do not outweigh the risks of raw milk consumption. Substantial data suggest that pasteurized milk confers equivalent health benefits compared with raw milk, without the additional risk of bacterial infections. The purpose of this policy statement was to review the risks of raw milk consumption in the United States and to provide evidence of the risks of infectious complications associated with consumption of unpasteurized milk and milk products, especially among pregnant women, infants, and children.
Although milk and dairy products are important components of a healthy diet, if consumed unpasteurized, they also can present a health hazard due to possible contamination with pathogenic bacteria. These bacteria can originate even from clinically healthy animals from which milk is derived or from environmental contamination occurring during collection and storage of milk. The decreased frequency of bovine carriage of certain zoonotic pathogens and improved milking hygiene have contributed considerably to decreased contamination of milk but have not, and cannot, fully eliminate the risk of milkborne disease. Pasteurization is the most effective method of enhancing the microbiological safety of milk. The consumption of milk that is not pasteurized increases the risk of contracting disease from a foodstuff that is otherwise very nutritious and healthy. Despite concerns to the contrary, pasteurization does not change the nutritional value of milk. Understanding the science behind this controversial and highly debated topic will provide public health care workers the information needed to discern fact from fiction and will provide a tool to enhance communication with clients in an effort to reduce the incidence of infections associated with the consumption of unpasteurized milk and dairy products.
Although pasteurization eliminates pathogens and consumption of nonpasteurized dairy products is uncommon, dairy-associated disease outbreaks continue to occur. To determine the association of outbreaks caused by nonpasteurized dairy products with state laws regarding sale of these products, we reviewed dairy-associated outbreaks during 1993-2006. We found 121 outbreaks for which the product’s pasteurization status was known; among these, 73 (60%) involved nonpasteurized products and resulted in 1,571 cases, 202 hospitalizations, and 2 deaths. A total of 55 (75%) outbreaks occurred in 21 states that permitted sale of nonpasteurized products; incidence of nonpasteurized product-associated outbreaks was higher in these states. Nonpasteurized products caused a disproportionate number (?150× greater/unit of product consumed) of outbreaks and outbreak-associated illnesses and also disproportionately affected persons <20 years of age. States that restricted sale of nonpasteurized products had fewer outbreaks and illnesses; stronger restrictions and enforcement should be considered.
There continues to be considerable public debate on the possible benefits regarding the growing popularity of the consumption of rawmilk. However, there are significant concerns by regulatory, or public health, organizations like the Food and Drug Administration and the Centers for Disease Control and Prevention because of risk of contracting milkborne illnesses if the raw milk is contaminated with human pathogens. This review describes why pasteurization of milk was introduced more than 100 years ago, how pasteurization helped to reduce the incidence of illnesses associated with raw milk consumption, and the prevalence of pathogens in raw milk. In some studies, up to a third of all raw milk samples contained pathogens, even when sourced from clinically healthy animals or from milk that appeared to be of good quality. This review critically evaluates some of the popularly suggested benefits of raw milk. Claims related to improved nutrition, prevention of lactose intolerance, or provision of “good” bacteria from the consumption of raw milk have no scientific basis and are myths. There are some epidemiological data that indicate that children growing up in a farming environment are associated with a decreased risk of allergy and asthma; a variety of environmental factors may be involved and there is no direct evidence that raw milk consumption is involved in any “protective” effect.
In October, I wrote a column for Veterinary Practice News (VPN) on the question of whether or not cancer is more common in dogs and cats now than it used to be. This is a core argument in the Truth About Pet Cancer propaganda video series I debunked HERE and HERE. The VPN article caught the attention of Dr. Bernadine Cruz, who asked me to visit her podcast to discuss the subject. Enjoy!
One of the most heartbreaking things we all see on social media are appeals for financial help to fund medical treatment. Especially here in the U.S., where healthcare is less readily available to low-income people than in most developed countries, it has become common to see crowdfunding campaigns raising money for medical care. It is inspiring that people are so often willing to help strangers with medical expenses, but it is sad and wrong that patients have to rely on such ad hoc methods for funding the care they need.
As sad as this inherently is, it becomes depressing and infuriating when these crowdfunding campaigns are intended to pay for unproven or quack therapies. Crowdfunding provides a new venue for people to be misled and exploited by proponents of untested, ineffective, and dangerous medical treatments, Now, not only the desperation of patients and their families are taken advantage of, but also compassion of well-meaning strangers who contribute to these campaigns.
Two recent studies have been published in the Journal of the American Medical Association (JAMA) investigating this issue, and these have been publicized through reporting by NPRand other media outlets.
More than 1000 medical crowdfunding campaigns for 5 treatments that are unsupported by evidence or potentially unsafe raised more than $6.7 million… These results reveal that a wide scope of cam- paigns for unsupported, ineffective, or potentially dangerous treatments are moderately successful in obtaining funding. Assuming that the funds raised are spent to pay for these treatments, donors indirectly contributed millions of dollars to practitioners to deliver dubious, possibly unsafe care.
The second study focused specifically on stem cell therapies and found similarly large amounts of money committed to campaigns for questionable treatment and also misleading appeals to donors:
Our search identified 408 campaigns seeking donations for stem cell interventions advertised by 50 individual businesses. These campaigns requested $7?439?308 and received pledges for $1?450?011 from 13?050 donors.
Crowdfunding campaigns for unproven stem cell–based interventions underemphasize risks and exaggerate the efficacy of these interventions. These findings suggest that medical crowdfunding campaigns convey potentially misleading messages about stem cell–based interventions. These claims may be especially powerful when embedded within compelling personal narratives.
As usual, there are no similar studies looking at how much crowdfunding there is for unproven and quack veterinary therapies, but it takes little time and effort to find such campaigns online:
Chi Chi has an integrated treatment plan that includes both traditional and holistic treatments…Chi Chi takes a number of traditional and Chinese medications to manage her medical conditions… and regular Hyperbaric Oxygen Treatments
the best course of treatment for quality of life and longevity is to go a TCM (Traditional Chinese Medicine) route. With a combination of a fully holistic/organic diet, herbal supplements, chinese medicine and an aggressive 3-day Vitamin drip protocol
Of course, I don’t believe the people making these appeals are doing anything wrong. They desperately want to help the animals they love, and they are willing to ask for help even when that may be difficult for them to do. And those who donate to these campaigns are illustrating the best qualities of the human spirit, compassion and concern for not only friends and family but complete strangers. Most of the appeals I have seen, including those that\ mention alternative therapies, do describe appropriate, science-based medical care, so hopefully these animals are getting the real treatment they need to get well.
Unfortunately, the fact remains that these animal owners and the good Samaritans who help them are paying for treatments that are at best questionable and, in many cases, clearly do not and cannot work. Though the practitioners offering them likely do so believing they are helping, at some point being a healthcare provider should mean knowing better and being required to provide effective treatment. It is hard not to wonder how many pets are harmed by the false belief in these therapies, and how much effective medical care could be paid for with the money that goes to unsupported or quack therapies.
I have been following with great interest the emerging evidence about grain-free and exotic protein diets as a possible risk factor for heart disease in dogs. I first raised the subject in response to several cases of dilated cardiomyopathy (DCM) I saw in my practice, and which became part of a study which has recently been published looking at the issue in this breed. There have been several other papers recently published touching on the relationship between diet and DCM in dogs, and I want to quickly discuss each of them
This is an excellent summary of what we know and don’t know about this issue so far. The bottom line is that a suspicious number of cases of DCM have been appearing in dogs eating what have been called BEG diets- boutique, exotic protein, grain-free. What this means is that diets without grains, diets with a high proportion of legumes, and diets with animal proteins that have not been traditionally used in dog food, and which consequently have not been studied as thoroughly in terms of their nutrient content and other factors, have been associated with DCM in a variety of breeds. This is not proof that the diets, or any particular characteristic of them, is causing this disease. Such proof will require different kinds of research studies. However, this is a potential warning sign that deserves to be acknowledged and followed up with appropriate research.
In some cases, the diets and disease has also been associated with a deficiency in the amino acid taurine. This is an amino acid that dogs do not normally require in the diet since they can make as much as they need. However, in some breeds there appear to be genetic factors that make individuals more susceptible to taurine deficiency, and associated heart disease. These may include reduced production of taurine, increased loss of taurine, or increased need for taurine. Certain diets that have low levels of the ingredients from which taurine is made or that contain substances, such as legumes and some types of. Fiber that make reduce absorption or synthesis of taurine and its precursors or that encourage taurine loss make act in con cert with these genetic factors to lead to deficiency and disease in some dogs. Many of the details in this hypothetical series of steps remain to be understood.
An example of how this problem may work comes from another recent paper looking at golden retrievers with DCM, including several of my patients.
In this study, the dogs with DCM had taurine deficiency, and most were eating BEG diets. Changing the diet and supplementing taurine, along with other treatments, seemed to improve or cure the disease in most, but not all of the dogs. Again, this was not a study designed to determine if the diets caused the taurine deficiency or the DCM, but the fact that all the dogs were on the diets that we are concerned about, and the fact that changing the diet and adding taurine, among other interventions, seemed to help most of these dogs, does make looking more closely at these diets worthwhile. It also makes it reasonable to consider avoiding these diets in golden retrievers, and perhaps other breeds known to have a higher-than-average risk of taurine deficient DCM even if we are not certain if the diets are the cause or, if so, how exactly that works.
It is important, however, not to get too fixated on taurine. Many of the dogs seen with DCM and eating BEG diets are not taurine deficient, so golden retrievers appear to be experiencing a different problem than these other breeds. It is possible that other aspects of these diets besides their effects on taurine levels could be a risk factor for DCM, and we know even less about how this might work.
This is illustrated by the third new study, which looked at dogs with DCM and evaluated the differences between those on grain-free diets and those on grain-based diets.
In this group of dogs, grain-free diets were associated with some signs of more severe heart disease than that exhibited by dogs on diets containing grains, though the differences did not appear in all measures of heart disease severity. None of the dogs in this group were taurine deficient, so whatever the relationship between diet and DCM here, it had nothing to do with taurine.
The great deal we don’t know about DCM and diet is frustrating to all of us. We have to try and resist the temptation, however, to substitute our own beliefs and theories for the missing facts. Proponents of grain-free and other unconventional diets will point to the gaps in our knowledge as evidence that we can’t really blame these diets and that there is no need to change what they feed. While it is true that we can’t be certain what role, if any, such diets are playing in causing heart disease, the fact that they are consistently associated with DCM in several different groups of dogs is, at the least, reason for concern and further research. What is more, none of the claims for the health benefits of grain-free and other unconventional diets have any compelling scientific support, so there is no good reason to choose such diets even if the evidence for their potential risks are still very preliminary.
Bottom Line We cannot say with certainty that BEG diets cause heart disease. We can only say that they have been associated with DCM in both golden retrievers with taurine deficiency and in other breeds without taurine deficiency. We can also say that changing diets appears to have benefitted some of these dogs, though many other treatments were employed at the same time, which limits out ability to know how important a factor this diet change was in the dogs’ recovery.
We can also say that none of the claims for health risks from grains in pet foods, or for health benefits from grain-free or other BEG diets, are supported by any reasonable scientific evidence. Certainly, the evidence for such diets is weaker than even the very limited evidence against them.
As pet owners and veterinarians, we need to proportion our confidence in any conclusions to the strength of the available evidence and be willing to change our minds as new evidence emerges. We also need to make our decisions now, even before we have perfect evidence. Right now, there is no solid reason to think grain-free diets have any health advantages, and there is weak evidence to suggest they might have health risks for some dogs. If you have a golden retriever, it seems reasonable to avoid the diets that have been associated with taurine deficiency and DCM in this breed. Even if you don’t have a golden, you should at least give some thought to why you might want to feed or avoid BEG diets. The evidence can’t make the decision for you, but it should certainly be considered.
I have written extensively about the subject of neutering (spaying and castrating male and female dogs and cats). The bulk of the discussion and debate about this procedure centers on the health effects. It is generally recognized to be a pretty safe procedure, though of course no surgery is entirely without risk. The scientific literature has limited information on the specific risks of the neutering surgery procedure itself and how often they occur.
Total complication rates for routine castration or spaying have been reported from 2.6%-33% of cases.The majority of these complications are minor and require no treatment. Complication rates vary considerably from practice to practice and are generally reported to be higher in studies of surgeries performed by students in training. Reported death rates are less than 0.1%.1-5
A new source of data on this subject has recently become available which represents the type of “Big Data” so popular these days. The Royal College of Veterinary Surgeons (RCVS) charity arm RCVS Knowledge, has a program in place that collects information from practices around the country in a central database. The goal is to encourage clinical audit, a quality improvement process in which veterinary practices can investigate the outcomes for their patients and compare these with those of other practices or with an established “gold standard.” This facilitates recognizing processes that aren’t working as well as they could and improvement in patient care.
The RCVS has recently released the results of data collection on complications of neutering. Though not the result of a controlled, prospective research process, this audit report is based on over 30,000 individual surgeries, so it at least represents a potentially powerful source of data. The specific variables that affect outcome of neutering surgery in individual animals can’t be identified, and there is the problem of patients who can’t be followed and whose outcome is unknown. However, this type of data complements the research evidence already available and gives us a general sense of the complication rates in the UK for these common procedures.
The outcomes measured were cases with no complications, those with minor complications not needing treatment, problems needing medical treatment, problems needing surgical treatment, and fatalities. About 8% of the cases in the database were not available for followup, and these were not included in the calculation of complication rates.
Total Overall Complications
Outcome
Frequency
Percent
Cum Percent
Abnormal but no treatment necessary
2795
9.3%
9.3%
Abnormal requiring medical treatment
2254
7.5%
16.8%
Abnormal requiring surgical intervention
341
1.1%
17.9%
Fatality of animal
29
0.1%
18.0%
No abnormality present
24627
82.0%
100.0%
Total
30046
100.0%
100.0%
Complications for Male Cats
Outcome
Frequency
Percent
Cum Percent
Abnormal but no treatment necessary
56
1.4%
1.4%
Abnormal requiring medical treatment
53
1.3%
2.7%
Abnormal requiring surgical intervention
23
0.6%
3.3%
Fatality of animal
3
0.1%
3.4%
No abnormality present
3885
96.6%
100.0%
Total
4020
100.0%
100.0%
Complications for Male Dogs
Outcome
Frequency
Percent
Cum Percent
Abnormal but no treatment necessary
977
11.4%
11.4%
Abnormal requiring medical treatment
796
9.3%
20.6%
Abnormal requiring surgical intervention
61
0.7%
21.3%
Fatality of animal
6
0.1%
21.4%
No abnormality present
6763
78.6%
100.0%
Total
8603
100.0%
100.0%
Complications for Female Cats
Outcome
Frequency
Percent
Cum Percent
Abnormal but no treatment necessary
616
7.0%
7.0%
Abnormal requiring medical treatment
385
4.4%
11.4%
Abnormal requiring surgical intervention
163
1.9%
13.3%
Fatality of animal
5
0.1%
13.3%
No abnormality present
7596
86.7%
100.0%
Total
8765
100.0%
100.0%
Complications for Female Dogs
Outcome
Frequency
Percent
Cum Percent
Abnormal but no treatment necessary
1146
13.2%
13.2%
Abnormal requiring medical treatment
1020
11.8%
25.0%
Abnormal requiring surgical intervention
94
1.1%
26.1%
Fatality of animal
15
0.2%
26.3%
No abnormality present
6383
73.7%
100.0%
Total
8658
100.0%
100.0%
These results are broadly similar to previously reported numbers, though lower than sometimes seen in studies in which inexperienced veterinary students are performing the procedures. They confirm that the procedure is very safe, that most complications are minor and do not require much, if any, treatment, and that mortality rates are very low. Females experience more complications because the surgery is necessarily more invasive. These data don’t tell us anything about the differences between specific neutering procedures, breeds, ages of patients, and many other factors, so they don’t let us predict the precise risk for individual patients. But they provide a general background that help us in making decisions about neutering.
References
Pollari FL, Bonnett BN, Bamsey SC, Meek AH, Allen DG.Postoperative complications of elective surgeries in dogs and cats determined by examining electronic and paper medical records. Journal of the American Veterinary Medical Association 1996;208(11):1882-6.
Howe LM. Short-term results and complications of prepubertal gonadectomy in cats and dogs. Journal of the American Veterinary Medical Association 1997;211(1):57-62.
Pollari FL, Bonnettt B.N. Evaluation of postoperative complications following elective surgeries of dogs and cats at private practices using computer records. Canadian Veterinary Journal 1996;37:672-8.
Burrow R, Batchelor D, Cripps P. Complications observed during and after ovariohysterectomy of 142 bitches at a veterinary teaching hospital. Veterinary Record 2005;157(26):829-33.
Root Kustritz MV. Effects of surgical sterilization on canine and feline health and on society. Reprod Domest Anim. 2012 Aug;47 Suppl 4:214-22.
Other myths about food allergies include the idea that changing diets can cause them (actually, prolonged exposure is usually needed to develop a sensitivity), that raw foods are less allergenic (nope, only more likely to give you a food-borne illness), and that you can use blood, hair, or saliva tests to diagnose food allergies (sorry, a limited ingredient diet trial is the only way to do this). This last misconception is perpetuated despite evidence from human medicine that it is not true because, quite frankly, it makes people money.
I’ve previously discussed an example of this quackery, Jean Dodds’ Nutriscan allergy testing system. In her book, Dr. Dodds provides many citations to support her claim that this is a legitimate test, but a cursory look at these shows they don’t make that case at all. And there are unpublished reports from at least one allergy specialist that suggest the test is not merely inaccurate but completely useless nonsense:
One veterinary dermatologist has performed her own uncontrolled test of Nutriscan, with Dr. Dodds’ knowledge and permission, and found it entirely unreliable. Twelve samples were submitted for testing in a blind manner, from dogs with known food sensitivities based on dietary testing, dogs with environmental allergies, dogs without allergic disease, and one sample of tap water. All samples including tap water, environmental allergy dogs, and normal dogs showed reactivity to beef, corn, milk and wheat. Some samples showed reactivity to soy. In some cases, these obviously false results would have led to recommendations against diets which actually helped these dogs.
Granted, this is essentially an unpublished anecdote, so while it counters the anecdotes Dodds and others put forward for Nutriscan, it is not published scientific research. Now, however, a different allergy test, using saliva and hair samples to identify allergies, has failed the same test as spectacularly as Nutriscan purportedly did.
Coyner K, Schick A. Hair and saliva test fails to identify allergies in dogs. J Small Anim Pract. October 2018. doi:10.1111/jsap.12952
Our study demonstrates that hair and saliva testing fails not only to identify allergic dermatitis in dogs, but fails to differentiate between animal and non-animal samples, providing essentially identical results, regardless of the origin of the sample.
These authors submitted not only hair and saliva from dogs with known allergies and dogs without allergies, but also fake hair samples from stuffed animals and water (in place of saliva). All of the samples tested positive for some allergies, and there was essentially no difference between the results and random chance.
Bottom Line
Saliva and hair tests for food allergies are a scam and a waste of time and money.
Back in 2011 I wrote about a therapy popular with alternative practitioners called prolotherapy. I try to check in from time to time to see if there is any new evidence for the treatments I consider, and in doing so I did find some new evidence. First, here’s my conclusion from the previous review:
Prolotherapy is a purported treatment for connective tissue and joint pain and disability. It involves injecting substances which induce inflammation and other chemical and cellular reactions into affected tissues. These reactions are theorized to relieve pain and improve function. The logic of this theory is questionable, and no clear mechanism for beneficial effects from prolotherapy has been described, but it is possible that the theory could be valid.
The clinical research on prolotherapy in humans is generally of low quality and results have been mixed. There is great variation in the techniques used by different investigators, so it is difficult to compare or generalize between studies.
There is virtually no controlled research investigating prolotherapy in companion animals, and all claims made for safety and efficacy in these species are based solely on anecdotal evidence.
The use of proltherapy in pets should be viewed as experimental with unknown risks and benefits. Such treatments should be reserved for patients that have significant symptoms that have failed to respond or cannot be treated by conventional means.
What Is It?
Prolotherapy involves injecting substances into joints or musculoskeletal tissue to treat pain and dysfunction. The particular substances used vary. Some are clearly useless (e.g. homeopathic remedies), but the evidence is growing that others may have some beneficial clinical effects. The most common substance currently used is dextrose, a form of sugar, but there are many others, and of course each substance has to be evaluated individually for specific uses.
Does It Work?
The in vitro and lab evidence suggests some potentially useful effects on joint tissues and in lab animals, but of course this level of evidence frequently turns out to be unreliable in predicting the actual effects in patients. At the time of my previous article, most systematic reviews were inconclusive, and the quality of the clinical trial evidence in humans was weak. There is still significant differences of opinions in different reviews, and all call for better quality evidence, but there is an emerging consensus that dextrose prolotherapy may be useful for arthritis in people. Other uses are still not supported by very convincing evidence. Here are some samples of the systematic review literature:
Limited evidence from low-quality studies indicates a beneficial effect of prolotherapy for OA management. The number of participants in these studies was too small to provide reliable evidence…Current data from trials about prolotherapy for OA should be considered preliminary, and future high-quality trials on this topic are warranted.1
Although anecdotal clinical success guides the use of prolotherapy for many conditions, clinical trial literature supporting evidence-based decision-making for the use of prolotherapy exists for low back pain, several tendinopathies, and osteoarthritis.2
This systematic review suggests that ST and PT may be effective treatment options for AT and that they can be considered safe. Long-term studies and RCTs are still needed to support their recommendation.3
Within the limitations of the study, dextrose prolotherapy may cause significant reduction in mouth opening and pain associated with TMJ hypermobility. Conclusions with regard to reduction of episodes of subluxation/dislocation cannot be drawn. There is a need of more high-quality RCTs with larger sample size and homogenous prolotherapy protocol to draw stronger conclusions on the effect of dextrose prolotherapy in patients with TMJ hypermobility.4
Dextrose injections decreased pain in osteoarthritis patients but did not exhibit a positive dose-response relationship following serial injections. Dextrose prolotherapy was found to provide a better therapeutic effect than exercise, local anesthetics, and probably corticosteroids when patients were retested 6 months following the initial injection.5
Use of dextrose prolotherapy is supported for treatment of tendinopathies, knee and finger joint OA, and spinal/pelvic pain due to ligament dysfunction. Efficacy in acute pain, as first-line therapy, and in myofascial pain cannot be determined from the literature.6
Moderate evidence suggests that prolotherapy is safe and can help achieve significant symptomatic control in individuals with OA. Areas for developing research Future research should focus on larger sample size, standardization of treatment protocol and basic science evidence.7
Overall, prolotherapy conferred a positive and significant beneficial effect in the treatment of knee OA. Adequately powered, longer-term trials with uniform end points are needed to better elucidate the efficacy of prolotherapy.8
Systematic review, including meta-analysis, and randomized controlled trials suggest that prolotherapy may be associated with symptom improvement in mild to moderate symptomatic knee osteoarthritis and overuse tendinopathy. Although the mechanism of action is not well understood and is likely multifactorial, a growing body of literature suggests that prolotherapy for knee osteoarthritis may be appropriate for the treatment of symptoms associated with knee osteoarthritis in carefully selected patients who are refractory to conservative therapy and deserves further basic and clinical science investigation for the treatment of osteoarthritis and tendinopathy.9
Unfortunately, the same proliferation of research evidence has not happened in veterinary medicine. To date, there is only one study of this treatment in dogs10 and none in cats.
Sherwood JM, Roush JK, Armbrust LJ, Renberg WC. Prospective Evaluation of Intra-Articular Dextrose Prolotherapy for Treatment of Osteoarthritis in Dogs. J Am Anim Hosp Assoc. 2017;53(3):135-1
This was a small but very high-quality study with appropriate blinding, randomization, control groups, and a mix of subjective and objective outcome measures. That’s the good news. The bad news is there was no significant difference between prolotherapy and placebo in any measure, so the therapy clearly didn’t work. This is only one study, and given the encouraging evidence in humans, it is possible that further studies will find some forms of prolotherapy helpful in veterinary patients.
Bottom Line There are a variety of theories behind prolotherapy, some more plausible than others, but there is not yet a clearly established general mechanism. The clinical trial research in humans is mixed and not robust, but there is moderate evidence supporting the effectiveness of prolotherapy for arthritis. There has only been one small animal study, a clinical trial in dogs for elbow and knee arthritis, and it found no benefit.
References
Krsti?evi? M, Jeri? M, Došenovi? S, Jeli?i? Kadi? A, Puljak L. Proliferative injection therapy for osteoarthritis: a systematic review. Int Orthop. 2017;41(4):671-679. doi:10.1007/s00264-017-3422-5
Rabago D, Slattengren A, Zgierska A. Prolotherapy in primary care practice. Prim Care. 2010;37(1):65-80. doi:10.1016/j.pop.2009.09.013
Morath O, Kubosch EJ, Taeymans J, et al. The effect of sclerotherapy and prolotherapy on chronic painful Achilles tendinopathy-a systematic review including meta-analysis. Scand J Med Sci Sports. 2018;28(1):4-15. doi:10.1111/sms.12898
Nagori SA, Jose A, Gopalakrishnan V, Roy ID, Chattopadhyay PK, Roychoudhury A. The efficacy of dextrose prolotherapy over placebo for temporomandibular joint hypermobility: A systematic review and meta-analysis. J Oral Rehabil. 2018;45(12):998-1006. doi:10.1111/joor.12698
Hung C-Y, Hsiao M-Y, Chang K-V, Han D-S, Wang T-G. Comparative effectiveness of dextrose prolotherapy versus control injections and exercise in the management of osteoarthritis pain: a systematic review and meta-analysis. J Pain Res. 2016;Volume 9:847-857. doi:10.2147/JPR.S118669
Hauser RA, Lackner JB, Steilen-Matias D, Harris DK. A Systematic Review of Dextrose Prolotherapy for Chronic Musculoskeletal Pain. Clin Med Insights Arthritis Musculoskelet Disord. 2016;9:CMAMD.S39160. doi:10.4137/CMAMD.S39160
Hassan F, Trebinjac S, Murrell WD, Maffulli N. The effectiveness of prolotherapy in treating knee osteoarthritis in adults: a systematic review. Br Med Bull. 2017;122(1):91-108. doi:10.1093/bmb/ldx006
Sit RW, Chung VC, Reeves KD, et al. Hypertonic dextrose injections (prolotherapy) in the treatment of symptomatic knee osteoarthritis: A systematic review and meta-analysis. Sci Rep. 2016;6(1):25247. doi:10.1038/srep25247
Rabago D, Nourani B. Prolotherapy for Osteoarthritis and Tendinopathy: a Descriptive Review. Curr Rheumatol Rep. 2017;19(6):34. doi:10.1007/s11926-017-0659-3
Sherwood JM, Roush JK, Armbrust LJ, Renberg WC. Prospective Evaluation of Intra-Articular Dextrose Prolotherapy for Treatment of Osteoarthritis in Dogs. J Am Anim Hosp Assoc. 2017;53(3):135-142. doi:10.5326/JAAHA-MS-6508

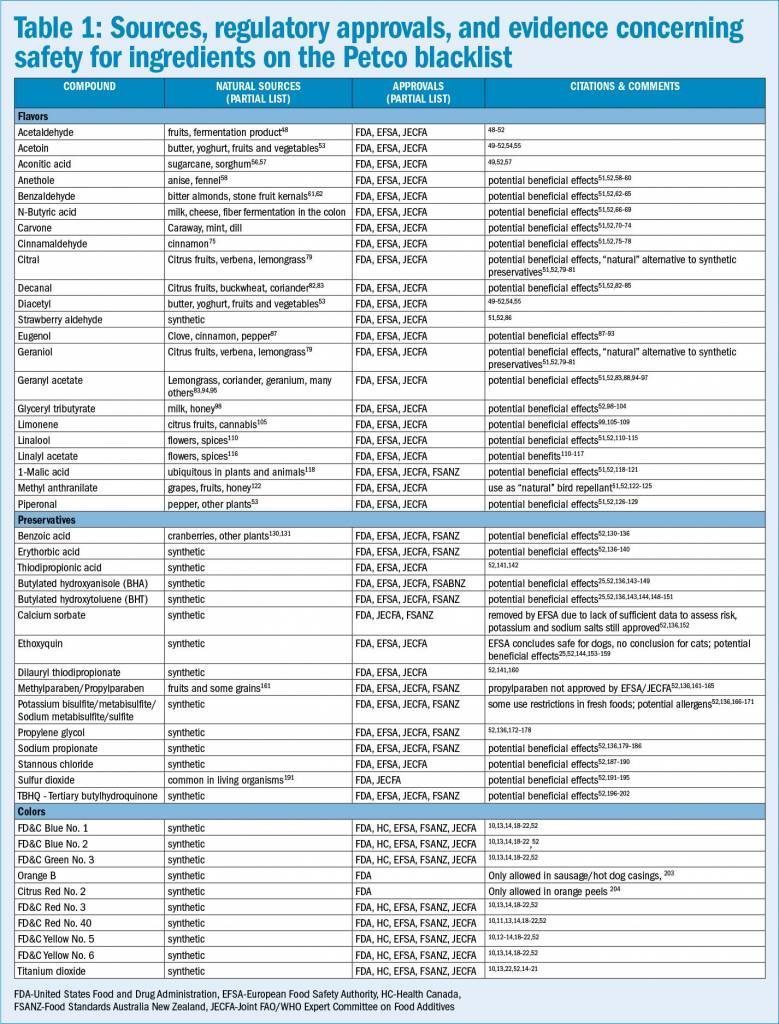






 0
0






 Set Youtube Channel ID
Set Youtube Channel ID
