Prompted by Dr. Hall’s recent assessment of the state of science-based medicine in Australia, I thought it was time to offer a “state of the profession” update on how science-based and evidence-based medicine in the veterinary field are doing in competition with opinion-based or faith-based medicine and outright woo. The situation resembles that in human medicine in many ways, of course, but the context is quite different, and that difference tends to put science-based medicine at a bit of a disadvantage.
The Context
The scale of the veterinary medical market is diminutive compared with that of human medicine. Perhaps the largest commercial player in veterinary pharmaceutical research, Zoetis (formerly a division of Pfizer) spent an estimated $400 million in 2013. By contrast, Pfizer itself has drastically cut its research budget for human medicines to a mere $6.5-7 billion for 2013. The difference in revenues is similar, and this provides less incentive for investment in the kind of research needed for truly science-based medicine.
The quality and quantity of research evidence in veterinary medicine is inevitably far lower than is commonly expected in human medicine, and consequently so are the standards of evidence clinicians and clients expect. Even with the best of intentions, we simply can’t expect to match the standards of our big-city cousin, human healthcare.
And due to the lesser societal value placed on animal health, except where it intersects with human health and the food supply, there is far less in the way of regulatory oversight of veterinarians. Most of the drugs we use, for example, are never licensed for the species or indication in which we use them. Off-label use based only sparse research or uncontrolled clinical experience is the standard.
Also, because animals are technically property, owners are free to do virtually anything they want to them. The application of almost any kind of quackery is completely legal under most circumstances. And even when there are rules about the claims and uses of a particular therapy, the understanding is that government will not enforce these unless there is a perceived direct impact on human health.
A recent example of this is the use of stem cell therapies in veterinary medicine. The FDA does not currently license any stem cell therapies for human use. The International Society for Stem Cell Research, which presumably consists of scientists convinced such therapies are very likely to prove safe and beneficial for at least some uses, still cautions people that the evidence for this is not yet available and that they should not seek out such therapies in countries where regulators do not prohibit them.
We have all heard about the extraordinary promise that stem cell research holds for the treatment of a wide range of diseases and conditions. However, there is a lot of work still needed to take this research and turn it into safe and effective treatments.
The International Society for Stem Cell Research (ISSCR) is very concerned that stem cell therapies are being sold around the world before they have been proven safe and effective.
Stem cell therapies are nearly all new and experimental. In these early stages, they may not work, and there may be downsides. Make sure you understand what to look out for before considering a stem cell therapy.
Remember, most medical discoveries are based on years of research performed at universities and companies. There is a long process that shows first in laboratory studies and then in clinical research that something is safe and will work. Like a new drug, stem cell therapies must be assessed and meet certain standards before receiving approval from national regulatory bodies to be used to treat people.
The evidence for the safety and efficacy of such therapies in veterinary patients is even weaker than that in humans, and yet stem cell therapies are widely marketed and in veterinary medicine. The FDA has jurisdiction over this practice, and the agency recently asserted its authority to require licensing of these products. However, even in the document claiming the right to regulate these treatments, the agency has indicated it is unlikely to do so when they do not clearly impact directly on human health or the food supply:
Although [autologous stem cell therapies] require [FDA approval], conditional approval or index listing to be legally marketed, FDA recognizes that these products pose a lower risk to human and animal safety than other categories of [stem cell therapy] when used in non-food producing animals and are, therefore, a lower enforcement priority.
The same understanding applies in most areas of veterinary medicine, so veterinarians are largely free to market any and all therapies without regulatory approval. While this may be necessary to ensure that therapies are available to veterinary patients in the absence of sufficient financial incentives to drive companies to seek licensing, it opens the door much more widely to woo than is generally the case in human medicine.
The Good News
The good news is that there are individuals and organizations in veterinary medicine committed to science and evidence-based practice. Efforts to promote this approach have grown dramatically in the last decade, and they are beginning to have an impact on at least the language, if not the underlying thoughts or actions, or practitioners. It is impossible to attend a veterinary continuing education conference without hearing titles like “An Evidence-Based Guide to Therapy X,” though the content is often less true to the principles and methods of EBM than such titles would suggest.
The organization I am most directly involved with is the Evidence-Based Veterinary Medicine Association (EBVMA). A small organization of about 75-100 people, promotes EBM at veterinary continuing education meetings, lobbies for incorporating EBM standards in research, publishing, clinical guidelines, and so on, and provides a small amount of funding (currently $1500/year) for research targeted at promoting evidence-based veterinary medicine.
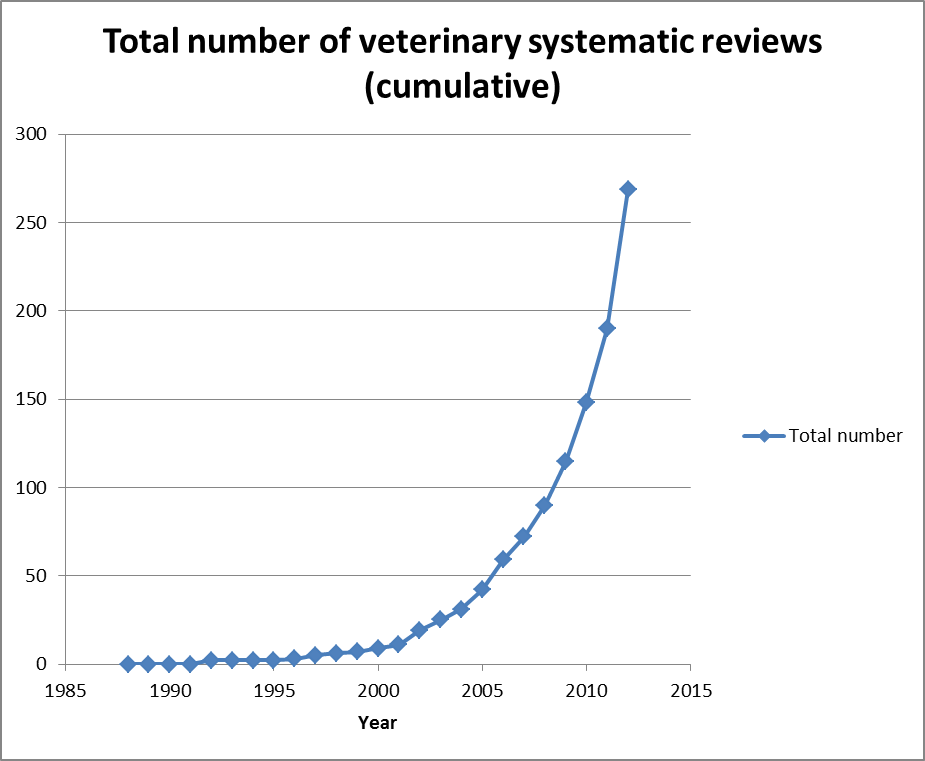
The Centre for Evidence-based Medicine (CEVM) at the University of Nottingham is a funded academic center aimed at conducting and supporting research to facilitate more evidence-based veterinary practice. The center has begun producing some very useful resources, such as a database of veterinary systematic reviews, and a small but growing collection of critically appraised topics for veterinary practitioners.
Such resources may seem rudimentary to physicians accustomed to much more voluminous and accessible synthetic literature, but these are essential first steps in helping veterinarians get accustomed to relying on science more and personal experience less. A recent study, for example, found that the number of systematic reviews in the veterinary literature has increased exponentially in the last ten years. It is still only a tiny number compared to the more than 5,500 systematic reviews produced by the Cochrane Collaboration alone by 2013, but it is a necessary start.
Perhaps the most exciting recent development in support of more science-based veterinary medicine has been the involvement of the Royal College of Veterinary Surgeons (RCVS) charitable arm in organizing and funding evidence-based veterinary medicine. The RCVS Knowledge group has offered grants in support of EBVM research and activities and has organized an international EBVM conference this fall.
In the absence of substantial government funding, private resources support most veterinary research. Industry is the largest player, including pharmaceutical companies, pet food companies, and the like. This money is, as I’ve mentioned, a tiny fraction of the equivalent R&D investments in human medicine, and it likely comes with the same risks of bias and other problems identified in human healthcare (though there is little research on this subject in veterinary medicine).
Private non-profit organizations and academic institutions make up most of the rest of support for the science behind veterinary medicine. As an example, the Morris Animal Foundation is the largest non-profit supporter of veterinary research, offering several million dollars annual in grant funding. Morris is currently funding the first longitudinal lifetime health study in dogs.
As in human medicine, most vets are probably shruggies; they practice mostly conventional medicine, but they think of themselves as “open-minded” and don’t see a problem with the integration of alternative therapies into routine practice. There is a bit of a cultural taboo, at least in the U.S., of criticizing the practices of other vets, so challenges to alternative practices often draw hostile responses not only from CAVM advocates but other veterinarians who don’t themselves offer alternative therapies. The notion that civil, substantive critique is essential to progress and the scientific method is not widely appreciated.
Science, and an evidence-based approach to practice, are only rarely specifically endorsed by veterinary institutions. Even fewer openly reject alternative therapies. The American Veterinary Medical Association, for example, used to have a policy on CAVM that stated:
The theoretical bases and techniques of CAVM may diverge from veterinary medicine routinely taught in North American veterinary medical schools or may differ from current scientific knowledge, or both.
The AVMA believes that all veterinary medicine, including CAVM, should be held to the same standards. Claims for safety and effectiveness ultimately should be proven by the scientific method… Practices and philosophies that are ineffective or unsafe should be discarded…Recommendations for effective and safe care should be based on available scientific knowledge and the medical judgment of the veterinarian.
Under pressure from CAVM advocacy groups, that has since been amended to remove any reference to science:
The AVMA believes that all aspects of veterinary medicine should be held to the same standards, including complementary, alternative and integrative veterinary medicine, non-traditional or other novel approaches.
- The foremost objectives in veterinary medicine are the health and welfare of the patient.
- Diagnosis and treatment should be based on sound, accepted principles of veterinary medicine and the medical judgment of the veterinarian.
- Veterinarians should have the requisite knowledge and skills for every treatment modality they consider using.
- A valid veterinarian-client-patient relationship must exist1.
- Owner consent1 should be obtained prior to initiating treatment.
- Medical records should include outcomes of treatment.
- Veterinarians should be aware of and abide by local, state, and federal statutes.
In contrast, the Australian Veterinary Association (AVA) has a policy rejecting any support for ineffective therapies generally, and specifically identifying homeopathy and homotoxicology as examples of such therapies:
Australian Veterinary Association (AVA) resources will not be used to promote therapies that, in the Board’s opinion, are not compatible with current understanding of physiology and pathophysiology and have been demonstrated to be ineffective by the current accumulated body of knowledge.
That the Board agreed that the veterinary therapies of homeopathy and homotoxicology are considered ineffective therapies in accordance with the AVA promotion of ineffective therapies Board resolution.
An attempt to pass a similar resolution in the AVMA was defeated overwhelmingly. Only a few other major mainstream veterinary organizations have taken formal positions on science and alternative medicine:
European Board of Veterinary Specialties
The veterinary profession received the prerogative for diagnosis and treatment of animal diseases based on the assumption that veterinarians are guided by scientific methods. The EBVS therefore only recognises scientific, evidence-based veterinary medicine which complies with animal welfare legislation Specialists or Colleges who practise or support implausible treatment modalities with no proof of effectiveness run the risk of withdrawal of their specialist status. No credit points can be granted for education or training in these so-called supplementary, complementary and alternative treatment modalities.
British Veterinary Association
The BVA cannot endorse the use of homeopathic medicines, or indeed any medicine making therapeutic claims, which have no proven efficacy. As with any medicine, BVA believes that veterinary medicinal products must be evidence-based, with any medicinal claims made by a manufacturer supported.
Federation of Veterinarians in Europe
[veterinarians should] work only on the basis of scientifically proven and evidence-based methods and to stay away from non-evidence-based methods.
The American Association of Veterinary State Boards (AAVSB), which is responsible for certifying continuing education (CE) courses for veterinarians taken in support of continued state licensure through the Registry of Approved Continuing Education (RACE), explicitly requires that subjects approved for RACE continuing education credit be based on sound scientific evidence, and the teaching of ineffective or unsafe practices cannot be approved as continuing education for veterinarians:
CE offerings shall be designed to…refresh the participant in the standards for practice and the foundational, evidence-based material presented in accredited colleges or schools of veterinary medicine… CE programs that advocate unscientific modalities of diagnosis or therapy are not eligible for RACE approval.
Furthermore, those programs that promote treatments known to pose significant risks, dangers that outweigh benefits or unproven effectiveness are generally not considered approvable. All scientific information referred to, reported or used in RACE Program Applications in support or justification of an animal-care recommendation must conform to the medically accepted and scientifically supported standards of experimental design, data collection and analysis.
This means in practice RACE will not certify most CAVM education. The Academy of Veterinary Homeopathy (AVH) actually sued the AAVSB to try and force them to accredit homeopathy CE courses. When this failed, CAVM proponents created their own CE accreditation organization to rubber stamp their own CE offerings, which unfortunately many states are accepting as legitimate.
Overall, the majority of veterinary medicine offered is at least compatible in theory with science-based medicine, though often the level of evidence available to support it is less than would be acceptable in human medicine. Most veterinarians stay away from the most egregious quackery, such as homeopathy and “energy medicine.” However, there is also bad news.
The Bad News
Apart from the serious lack of adequate scientific evidence to support even most mainstream veterinary practices, questionable or outright quack practices are widespread and appear to be growing in acceptability and popularity. Some of this reflects similar trends in human healthcare. People often begin to inquire about dietary supplements, herbal remedies, acupuncture, and chiropractic, as well as even more dubious practices, for their pets after having employed them for themselves or heard encouraging anecdotes from friends and family. While there is not any formal research evaluating the popularity of CAVM treatments, subjectively they certainly appear to be infiltrative academia and general practices at a frightening pace.
A large part of the credit/blame for this likely belongs to CAVM advocates, who are far better organized and funded, and far more aggressive than proponents of EBVM. The American Holistic Veterinary Medical Association (AHVMA) and its associated fundraising arm the American Holistic Veterinary Medical Foundation (AHVMF) have proven very successful at promoting CAVM and paying lip service to science and EBVM while clearly being interested only in promoting what they already believe without, or despite the scientific evidence. They promote the most ridiculous quackery at their CE meeting, like “Earth Acupuncture” to heal the planet, dowsing, and of course homeopathy, Traditional Chinese Veterinary Medicine, Reiki, and all the others. Yet they have managed to raise over $1 million in the last year to promote “research” and teaching of alternative veterinary therapies. By the standards of veterinary medicine, this is not small change!
Much of this money has been given to veterinary colleges in the form of grants to support teaching and research activities by dedicated CAVM proponents. The University of Tennessee, University of Florida, and University of Louisiana veterinary schools have received large grants and have become the leaders in veterinary quackademic medicine as a result. The comments of the leaders of the AHVMA and AHVMF make it clear this money is intended not for any kind of rigorous research evaluation of plausible CAVM practices, but simply to promote these and give them a patina of scientific legitimacy.
The AHVMA and AHVMF also organize student alternative medicine clubs at veterinary colleges and offer scholarships and other support for students wishing to study CAVM methods. The influence of this on what will be considered mainstream, legitimate medical practice in the future is potentially significant, and quite disturbing.
Apart from their fundraising success, these two organizations have been able to infiltrate and influence mainstream veterinary organizations. Along with the American Academy of Acupuncture, the AHVMA has been admitted to the governing body of the American Veterinary Medical Association. Perhaps not coincidentally, this organization effectively lobbied to kill the resolution in the AVMA House of Delegates to declare homeopathy an ineffective therapy. The AVMA statement on CAVM was also amended to remove any talk of science or scientific evidence at about the same time the AHVMA was admitted.
There are, of course, many other CAVM organizations also proselytizing and marketing their particular brand of alternative medicine. In addition to the organizations of homeopaths and acupuncturists, there are national and international academies and associations for veterinary chiropractic, traditional Chinese medicine, naturopathy, herbal medicine, pet psychics (sorry, “animal communicators”), and pretty much any other variety of alternative medicine you can imagine. And all of them offer certifications which, though not recognized by the official AAVSB, are indistinguishable from real, meaningful credentials to pet owners and most regular veterinarians. And all of these groups raise money, lobby, and otherwise promote their own brands of woo and most of the others at a volume that cannot be matched by advocates of EBVM and science-based medicine.
The internet is, of course, the Wild West for quack therapies. Claims are made for miracle treatments that are not only unsupported or unquestionably ridiculous but blatantly illegal. The FDA, FTC, and other relevant agencies almost never take any action, so it is very much a buyer-beware marketplace. The vast majority of the health information available to animal owners on the internet is marketing from someone with a product or practice to sell. I play whack-a-mole here as best I can with the most egregious misinformation, and a few others do the same, notably fellow SBM contributor David Ramey. But this is a mere drop in the CAVM propaganda ocean.
Where Do We Go From Here?
It is difficult to see the situation in veterinary medicine with respect to quackery improving any time soon. The resources, passion and momentum, and political environment all appear to favor the greater infiltration of alternative therapies into the mainstream of veterinary practice. The development of evidence to validate or invalidate the plausible among CAVM treatments is glacial. And the culture of veterinary medicine favors extreme individual autonomy and discourages open criticism and debate on the subject.
Professional institutions, such as the AVMA and specialty boards, are reluctant to criticize or discourage any practice that veterinarians can legally sell or to take any position on what constitutes scientifically legitimate medicine. And academic, research, and teaching institutions appear to be opening their doors to CAVM, with the hinges greased by contributions from the CAVM lobby. This raises the specter of the next generation of veterinarians being taught that homeopathy, energy medicine, and similar nonsense is legitimate, respectable, even “evidence-based” veterinary medicine.
Fortunately, there are organizations and individuals who see the problem, the danger the philosophy and practices of alternative medicine represent to our patients and our profession, and who are making an effort to stem the tide. SBM has had significant impact on the discussion or CAM in human medicine, and to a lesser extent those of us advocating for science-based medicine in the veterinary domain are attempting to do the same in our field.
At a minimum, continuing to challenge the claims of CAVM proponents mars their efforts to make their practices seem uncontroversial or ordinary and legitimate. Our efforts to highlight the facts may save at least some animal owners from being misled or buying into unproven or quack therapies. And perhaps we may even influence the next generation of vets ourselves, and sustain the skepticism needed to resist CAVM narratives.
Though the current state of science-based veterinary medicine is a bit shaky, there is hope. I encourage anyone interested in defending animals and animal owners from CAVM to get involved in one of the organizations I mentioned that are defending evidence-based veterinary medicine. Make it clear to your clients and colleagues, if you are a veterinarian or veterinary technician, or to your vet if you are an animal owner, that that science-based and evidence-based medicine are the right approaches to animal care, and that CAVM is not a safe, effective, or ethical alternative. Ask for evidence whenever a claim is made, and demand more than personal experience and testimonials.
And if you can, contribute not only your time and energy but financial support. Donations to non-profit groups supporting real research, like the Morris Animal Foundation, or promoting evidence-based medicine, can help balance the resources currently pouring into veterinary medicine in support of CAVM. And your choices of where you spend your money as an animal owner can make a difference too. Some vets offer CAVM because they believe in it. Plenty of others offer it becomes it sells! Make sure your vet knows that you want to pay for science-based care, not untested and implausible products and services or outright quackery.






