Stookey GK. Soft Rawhide Reduces Calculus Formation in Dogs. Journal of Veterinary Dentistry. 2009;26(2):82-85. doi:10.1177/089875640902600202
Hennet P. Effectiveness of an Enzymatic Rawhide Dental Chew to Reduce Plaque in Beagle Dogs. Journal of Veterinary Dentistry. 2001;18(2):61-64. doi:10.1177/089875640101800201
Hooda S. In vitro digestibility of expanded pork skin and rawhide chews, and digestion and metabolic characteristics of expanded pork skin chews in healthy adult dogs, Journal of Animal Science, Volume 90, Issue 12, December 2012, Pages 4355–4361, https://doi.org/10.2527/jas.2012-5333
Christine Arhant, Rebecca Winkelmann, and Josef Troxler. “Chewing Behaviour In Dogs – A Survey-based Exploratory Study.” Applied animal behaviour science, v. 241 ,. pp. 105372. doi: 10.1016/j.applanim.2021.105372
Bellows J, Berg ML, Dennis S, Harvey R, Lobprise HB, Snyder CJ, Stone AES, Van de Wetering AG. 2019 AAHA Dental Care Guidelines for Dogs and Cats. J Am Anim Hosp Assoc. 2019 Mar/Apr;55(2):49-69. doi: 10.5326/JAAHA-MS-6933.
Harvey CE, Shofer FS, Laster L. Correlation of Diet, Other Chewing Activities and Periodontal Disease in North American Client-Owned Dogs. Journal of Veterinary Dentistry. 1996;13(3):101-105. doi:10.1177/089875649601300304
If you are interested in canine and feline aging, I have a new continuing education course available on the Veterinary Information Network (VIN). Two hours of a pre-recorded self-study course and two hours of live, interactive sessions focusing on:
Session 1 (self-study) Introduces key geroscience concepts and core physical, function, behavioral, and metabolic changes in aging dogs and cats
Session 2 (self-study) Covers the concept of frailty, reviews significant clinical disorders in geriatric dogs and cats, and begins looking at what we can do about aging
Session 3 (August 9, 2023 5pm PDT) Introduces specific clinical assessment tools and case study examples for the independent practice exercise
Session 4 (August 30, 2023 5pm PDT) A review of the case examples and course wrap-up
This is the proceeding summary and the slide deck from my presentation on Nutrition and Aging at the 2023 ACVIM Forum in Philadelphia.
Effect of Nutritional Interventions on Aging
INTRODUCTION While the clinical phenotype of aging is readily identifiable, a precise definition of this ubiquitous phenomenon is challenging. A useful pragmatic definition is the accumulation of changes over time that increase an individual’s susceptibility to disability, disease, and death. The passage of time is a key factor, yet it is not the primary driver of aging. Factors such as genetics, environmental exposures, and nutrition also play critical roles.
The cellular and molecular changes characteristic of mammalian aging are often grouped into categories known as hallmarks of aging (Figure 1).1 Though not exhaustive, this scheme provides useful starting points for investigations into the mechanisms of aging and for evaluation of interventions to influence this process and mitigate the negative health outcomes resulting from it.
Figure 1. Hallmarks of aging.1
The scientific understanding of these hallmarks, and how they can be manipulated, has reached a point at which aging can reasonably be viewed as a modifiable risk factor for disability, disease, and death. The length of time an individual lives (lifespan) and the proportion of that life free of significant age-associated disability or disease (healthspan) can be extended by targeting the underlying mechanisms of aging.
Interventions so far demonstrated to increase lifespan and healthspan in animal models include modifications of activity level and environmental conditions, pharmaceuticals, and diet.
There are various ways in which diet can potentially impact health and longevity-
Dietary interventions to prevent and treat age-associated disease (e.g. dietary therapy of chronic kidney disease in cats)2
Optimization of diet to match changing nutritional requirements throughout the lifecycle (e.g. differences in the protein content of diets formulated for puppies and for geriatric dogs)3
Optimization of diet for individual health (e.g. potential applications of nutrigenomics and metabolomics)4
Extension of lifespan and delay or prevention of age-associated disease through dietary interventions targeting specific hallmarks of aging
The last approach has been the focus of extensive research since at least the early twentieth century, when it was first shown that reduced food intake extend lifespan in rats.5 The field has progressed from rather crude, trial-and-error methods to the evaluation of specific cellular and molecular mechanisms that can be stimulated and inhibited to achieve substantial changes in median and maximum lifespan and in health. The primary, though by no means only, hallmark of aging targeted by dietary interventions is dysregulated nutrient sensing.6
NUTRIENT SENSING AND AGING Nutrient sensing involves a complex network that detects the availability of nutrients and energy and regulates cellular growth and metabolism, apoptosis and autophagy, protein synthesis, and other processes depending on the available nutritional resources. The functioning of these mechanisms changes in a consistent pattern with aging, though the rate of this change differs between species and even between individuals. These changes are a key element in the degenerative process of aging and the increasing susceptibility to disease and death.
Critical pathways maintaining an appropriate balance between the energy and nutrients taken in and the function and maintenance of an organism are highly conserved across organisms as evolutionarily distant as flatworms, fruit flies, rodents, dogs and cats, and humans. An example is the target-of-rapamycin (TOR) protein kinase, homologues of which regulates cell proliferation, protein synthesis, and many other anabolic processes in yeast just as in mammals.5,6
A recurring motif in aging biology is that nutritional stress, such as reduced availability of calories or specific nutrients, can suppress some nutrient sensing pathways and activate others, with a net effect of inhibiting age-related disease and extending lifespan. These pathways are complex and interact extensively with each other and with many other physiologic processes, so simple generalizations are inherently problematic. However, sufficiently consistent patterns have emerged in a variety of organisms to allow a broad but useful characterization of some key elements and their influence on lifespan and healthspan when activated or suppressed by dietary interventions. Table 1 provides a brief list of some key regulators in these pathways and their typical impact on lifespan when activated or suppressed.
Table 1. Key regulators of nutrient sensing pathways.
Regulator
Activities
Effects on Lifespan
“Bad Guys”
mTOR (mechanistic target of rapamycin)
Increases cell growth, cell division, protein synthesisPromotes anabolism
Activity increases with ageHigh activity promotes aging and age-related diseaseSuppression increases lifespan
High activity reduces lifespanSuppression increases lifespan
“Good Guys”
AMPK (AMP-activated protein kinase)
Promotes catabolism and suppresses anabolismSuppresses mTORStimulates FOXO and SIRT
Activity declines with ageHigh activity increases lifespan
FOXO (forkhead box O transcription factors)
Coordinates nutritional stress responseRegulates energy metabolism, cellular proliferation and apoptosis, redox balance, autophagyInhibits mTOR
High activity increases lifespan
SIRT (NAD+-dependent sirtuin deacetylases)
Regulates energy metabolism and balance between anabolism and catabolismInhibits mTORStimulates FOXO
High activity increases lifespan
DIETARY INTERVENTIONS TO INCREASE LIFESPAN
Caloric Restriction (CR) Defined as significant reduction in calorie intake (typically 20-50%) without malnutrition or change in macronutrient ratios, CR has been consistently shown to increase lifespan and reduce the burden of age-related disease in multiple species, including rats and mice, primates, and dogs.5,7,8 The effects of this intervention are broad, but suppression of mTOR and activation of AMPK and SIRT are considered central mechanisms in this approach.6,9 Pharmacologic CR mimetics targeting these mechanisms have also extended lifespan and healthspan in some studies.10
CR is the most consistently effective dietary intervention for extending lifespan and healthspan. However, there are limitations to this approach. Some studies involved concurrent protein restriction or control animals with obesity and metabolic dysfunction, which complicates determination of the true effect size of pure CR. Genetic background also influences the impact of CR, and some strains of mice show no benefit or even reduction in lifespan.5 Such an extreme intervention is also too impractical and potentially dangerous for routine use in humans or companion animals.
Protein and Selective Amino Acid Restriction Rodent studies have demonstrated extension of lifespan with general protein restriction and with selective restriction of sulfur-containing amino acids (e.g. methionine, cysteine) and branched-chain amino acids (BCAA; e.g. leucine, valine). Some of these have also involved CR, but benefits have been seen with isocaloric protein and amino acid restriction, though the effect size is considerably smaller than that of CR. Inhibition of GH/IGF-1 and mTOR appear to be the main mechanisms for this effect.5,11
Timing of Feeding Manipulations of the timing of feeding, including fasting regimes, time-limited feeding, or cyclic intermittent CR have all been shown to extend lifespan. Most of these regimes amount to a form of CR, but they may be more sustainable in real-world use. A few studies of isocaloric manipulations of the timing of feeding have also shown positive effects on glucose, insulin, and IGF-1 and the induction of short-term ketosis, all of which might have beneficial effects on lifespan and healthspan, though this has not be conclusively demonstrated.5
Ketogenic Diets (KD) Carbohydrates-restricted diets which induce ketogenesis, as well as direct administration of some ketone bodies, have been shown in a few studies to increase lifespan and healthspan in mice and invertebrate models of aging. Such diets may mimic the effect of CR in shifting metabolism away from glycolysis and towards fatty-acid oxidation. Some KD formulations may also be protein-restricted and inhibit mTOR activity. The evidence supporting the effect of KD on longevity, however, is currently quite limited.
DIETARY INTERVENTIONS FOR LONGEVTIY IN COMPANION ANIMALS Extension of lifespan and healthspan by CR has been demonstrated in dogs, and there is some limited evidence that other dietary manipulations might increase longevity in cats.7,12 However, the potential impact of CR, protein restriction, and ketogenic diets on aging in companion animals is largely unknown, and most strategies are based on speculation and extrapolation from research in rodents or other laboratory animals.
Unfortunately, strong claims for lifespan extension have been made for various dietary interventions, including raw diets, “fresh food,” and ketogenic diets. These claims are not based on robust, target-species research and present a misleading picture of the state of the science in this area. The belief that an optimal diet for longevity is known and can be formulated for dogs and cats, or even for individual animals, is unjustified and places an unfair and unsupportable burden on pet owners to choose the “right” food.
Future studies investigating the hallmarks of aging and their response to dietary manipulations as well as clinical studies directly assessing the impact of novel feeding strategies on lifespan and healthspan are needed before clinical recommendations regarding diet and longevity can be made with confidence. Until that evidence is available, it is most appropriate to continue offering current, evidence-based dietary recommendations.
REFERENCES
1. López-Otín C, et al; Hallmarks of aging: An expanding universe. Cell 2023;186(2):243.
2. Ross SJ, et al; Clinical evaluation of dietary modification for treatment of spontaneous chronic kidney disease in cats. J Am Vet Med Assoc 2006;229(6):949.
3. Laflamme DP; Nutrition for aging cats and dogs and the importance of body condition. Vet Clin North Am Small Anim Pract 2005;35(3):713.
4. Ordovas JM, et al; Personalized nutrition and healthy aging. Nutr Rev 2020;78(12 Suppl 2):58.
5. Lee MB, et al; Antiaging diets: Separating fact from fiction. Science 2021;374(6570).
6. Pignatti C, et al; Nutrients and Pathways that Regulate Health Span and Life Span. Geriatr 2020;5(4):1.
7. Lawler DF, et al; Diet restriction and ageing in the dog: major observations over two decades. Br J Nutr2008;99(4):793.
8. Pifferi F, et al; Caloric restriction, longevity and aging: Recent contributions from human and non-human primate studies. Prog Neuropsychopharmacol Biol Psychiatry. 2019;95.
9. Green CL, et al; Molecular mechanisms of dietary restriction promoting health and longevity. Nat Rev Mol Cell Biol. 2022;23(1):56.
10. Madeo F, et al; Caloric Restriction Mimetics against Age-Associated Disease: Targets, Mechanisms, and Therapeutic Potential. Cell Metab. 2019;29(3):592.
11. Brandhorst S, et al; Protein Quantity and Source, Fasting-Mimicking Diets, and Longevity. Adv Nutr. 2019;10(Suppl 4):S340.
12. Cupp C, et al; Effect of Nutritional Interventions on Longevity of Senior Cats. Int Jounrla Appl Res Vet Med. 2007;5(3):133.
Back in February, I announced that I had received the VIN Veritas Award in recognition of my efforts to promote science-based pet health and combat misinformation about veterinary medicine. Subsequent to that announcement, I have also received a lot of kind and supportive comments from people who have found my work here useful. That has always been my only goal, and I am very grateful to know that the blog has helped so many people.
Of course, one of the nice things about such recognition and feedback is that it helps to balance the steady stream of hate mail that is an inevitable consequence of challenging people’s beliefs and assumptions publicly. I have grown a pretty thick skin in the 14 years since I started the SkeptVet Blog, but I do keep track of this feedback as well. I don’t of course, provide a platform here for people to vent their anger or disinformation since that would be counter to the very purpose of the blog, and there are plenty of other places people are free to rant away unhindered.
However, I do periodically post anonymized selections from this collection. Here are the previous selections-
While some comments are just bizarre enough to be entertaining, the main reason to do this is to remind the more reasonable readers that such intense anger and pervasive misconceptions are not rare and that there is still a critical need for more and better public communication about science and medicine. These selections also highlight some of the leading concepts that underlie the popularity of unproven or ineffective treatments. These include-
The mistaken belief that anecdotes can prove what causes or cures disease and that controlled scientific research is unnecessary or no better than opinion
The only way to “know” if a therapy works is to try it and “see for yourself,’ and if you do this then scientific research is pointless
That expertise is meaningless and just a form of ideological or financial bias or an attempt to suppress truth and control people
That “research” is just people haphazardly searching for opinions and evidence that support their beliefs, and that doing such “research’ makes one’s views as reliable and informed as a formally trained “expert.”
These are all expressions of core cognitive biases that none of us are free from. No amount of information can overcome the power of such biases unless we first have the humility to recognize we are vulnerable to them and that formal methods for reducing bias and error (aka science) work better than personal experience of trial and error. This is the core message that has to be understood before anyone enamored of unscientific practices will even begin to see contrary scientific evidence as a reason to question their own beliefs.
I have to admit I feel that the problems this blog aims to address have only gotten worse since I began writing it. That doesn’t make the effort meaningless, as all the kind comments I have received in the last couple of months attest. But it does mean the effort must continue and must grow. More and more scientists should participate in the public conversations and debates about the nature of scientific information and pseudoscience or anti-scientific misinformation. We are well beyond any time in which bizarre fringe ideas could be ignored. The fringe has a way of becoming mainstream even when it remains bizarre and disconnected from reality. We have seen the very real harm that leads to over the last few years, and if ever there was a time to push back against the dismissal or distortion of science, it is now!
I have left all the typographical quirks of the comments as they were posted or emailed, and organized them into broad categories reflecting the major themes. Enjoy (and learn)!
But it Worked for ME!
I’ve been using Essiac for several months. I’ve known about it for several years. All I can say is it DOES work!… Obviously, bigP and Doctors don’t want you to believe that God’s medicine works! It’s NOT snake oil…1,000 and 1,000 of people don’t lie. But science always lies!…How dare you assume we liars.
People can do a study of one and document their experience. This is not “anecdotal evidence”, it is scientific. If treatment coincides with a cessation of symptoms, discontinuation coincides with a recurrence of symptoms, and this process can be repeated, that is scientific evidence that the treatment is effective. Note that I said evidence, not proof. Proof doesn’t seem to exist anymore. Also, placebos have immense value. Why not let them be if they appear to be helping? Why are you so eager to burst people’s bubbles?
Nutriscan worked for my dog…My dog had Inflammatory Bowel Disease, Jean’s test showed he is allergic to 19 out of 24 foods….He now is FREE of IBD, with no surgery and no lifetime on drugs.
Homeopathy is incredibly effective. There are many scientific studies in India and elsewhere proving its effectiveness, which you will naturally close your eyes to. The irrational, dogmatic yoke of the allopathic system and it’s mindless religious adherents who shriek in terror whenever their brainwashing is threatened is what boggles the mind.
You do not have all the answers….Our bodies are not only made up of matter, but they’re also made up of energy. We can use that energy to diagnose and treat disease. Just because there hasn’t been a scientific study to prove it, doesn’t mean for one minute that it’s not so. I was skeptical. I didn’t expect any results. But, I’m telling you a CranioBiotic technique worked on my body within hours and eventually cured me of an illness many are suffering with
Dr Jones is a Saint for holistic methods. You can process your opinions until Hell freezes over but you cannot dissuade those of us who have been blessed by Dr Jones & his unrelenting desire to help pet owners.
You are flat refusing to believe that anything outside of your facts could be true…I know in your opinion that just counts as anecdotal evidence, not fact, but it’s a fact.
As a homeopath for more then 20 years, I know it works, and so much better then allopathic medicine. Before you poo poo homeopathy, study it…, until you do this, I know your wrong.
No, they don’t! They try and give your dog every vaccine known to man every year!! And yes, the lifespan of dogs has absolutely gone down!! Everything you said is backwards!!
Horrible article, one-sided and arrogant. My dachshund was irreparably damaged by a vaccine, as was my daughter. Science does not thrive with the blind adherence to YOUR type of misinformation, driven by greed. Thank God the ineffective and dangerous Covid vaccine is going to blow this false, profit driven narrative wide-open!
Traditional Chinese Medicine has been around several thousand years and has served both humans and animals very well, without double blind studies, peer- reviewed articles etc. It’s only thanks to the Rockefeller and Rothchild families that modern medicine has decided these are necessary. A paradigm shift is well overdue.
Anecdotal Evidence is pretty much people stating what they have used that has worked for them. When there are thousands of people stating the same thing it is usually accurate!! I believe what these thousands of people say MUCH more than I believe studies that are done to the corporate worlds specs to achieve the results that the corporate world wants, and if the study shows results that the corporate world does not like, they simply end the study and start again with a modified study that will show what they want even if the results are grossly deceptive!!!
Sorry… great article up till your baseless comment on raw food. Please do more homework and gain some personal experience with raw before scaring readers
Shill for Big Pharma, Big Kibble, etc.
It does make me wonder if you are paid by the Big Pharma companies as this is what pays for the ‘scientific research papers’ to back Conventional Medicine;
This writer sounds exactly like the pharmaceutical companies… Why? To protect profits. Billions and billions of dollars in profits. And this article reeks of profit-protection scare-tactics. Bottom line (to the writer): You’re trying way too hard. After reading your article I did a few minutes research on colloidal silver. Is it a miracle drug? No. But is it snake-oil? No. Is skeptvet desperately trying to steer/scare the reader away from colloidal silver? Yes.
skeptvet. Just another useless quack from the pharmaceutical companies that try to sell his vaccines and bullshit chemical induce medicine that kills everything and one on this planet, and doesn’t work at all. You are the real quack hear.
Please, you main stream vets are a joke. Selling”prescription” diets with low quality ingredients all the while filling your pockets to the max. This has gone on way to long. After all, you cant sell meat bought at a grocery. Now there’s a concept. Real meat for dogs wow. Your time has come!!
I am a vet student- how they teach you to keep your pet healthy is actually scary. what they teach you is how to cut into your pet, how to remove tumors, how to give chemo, how to make money…
You are not listening. You can’t. You shouldn’t be near animals. After trusting vets and spending over 10000$ ….i don’t give a crap about your so called clinical trials.
You are obviously a quack…. This guy is a being paid by someone to spread this disinformation.
Vaccines are promoted by big pharma to sell more drugs and inces the millions of dollars the CEOs make.
Who the fuck is the QUACK that published this article…….and who paid for you assanine services…… If you want to call it that? Furthermore what dog food company do you work for? Lol
You sound like you might also get kickbacks from the fossil fuel industry by peddling windmill cancer, mister vet. Empaths: discern the drive behind this website. Anyone else getting the pharma vibe here?
Good luck, mister “vet”. The world is waking up. Let go or be dragged, dear.
Are you sponsored by the AMA or a pharmaceutical company?
how you still decide to defend kibble is BEYOND me. is Royal Canin making you do this post? Lol
Every field wants to squash any competitive field when dollars are at stake
Dear Skeptvet, you also come across as very biased. When I read your posts there is a consist thin veil and right underneath is always support for the meat industry like they the FDA and USDA are always doing what is right. Give me a break. I have been left wondering, after reading your review, how much of your education and training has been funded by the meat industry.
Sorry but vet like you only look for the money not for the health of our animals.
Skeptvet is obviously a shill for big pharmaceuticals or is just recklessly ignorant.
You’re a vet who stands to lose a lot of money in your own ineffective cancer treatments and surgeries. If people found out about a cheap herbal alternative that actually cures cancer, you’d go out of business, just like the medical mafia cartels. I trust nature over educated fools.
Logic?
There are those who are religious who insist that only their religion is the true one. However, commonsense alone says they can’t all be right – or can they in some fashion?
Lucky your not English you may be in the Tower of London, by calling our Queen a witch. The Royal family The a Queen Morher and our own dear Queen both users of homeopathy for there medical care, and look how well they have lived…. God Bless you and may the Holy Spirit fall in you.
Lol, your incompetence is showing. If you took this much time to unnecessarily write something like this, imagine putting effort into actually helping someone. This just screams that you find a competitor threatening because they practice a different method of healing.
All I can say is Science fails us thus we turn to other ideas that sound more logical and when we see positive results in our pets we are satisfied….Scientists are so adamant about studies and more studies.. then what studies have they DONE and what are the results? People and their pets are all disposable.. population control seems to be the true goal in the Scientific world.
I love you skeptvet, even though you are probably a machine! You are proof at how one-sided and close minded ‘science’ can be. Ha! It’s laughable.
Your fear of unpasteurized milk is causing you to form an opinion based on cherry picking evidence as “facts” that changes the trajectory from “Science” to fear mongering germaphobe jargon to form or change a person’s opinion. I’m a diabetic, drink grass fed raw milk through many stages of my life, and here I am doing great! Just live your life. stop trying to control people. Funny you source FDA links, because they are responsible for more deaths than any war.
LOL vaccines extend a pets life, hahaha more like the opposite in actuality…I guess as a ‘skeptical vet’ we know what side of the fence you’re on…the one for veterinarians who are ‘general practitioners’ of fake bandaid medicine vs those who better understand the holistic approach of more natural remedies that aren’t full of toxins or bandaid solutions
Sir, your not doubting these people’s stories, your doubting God’s abilities for ‘He created all things’, therefore he also created ways for the body to natural heal itself with proper nutrients. These herbs are pasted down from generations of ancestors. ….That is science! ….
don’t be so naive as to believe anything from the FDA. they are completely corrupt, like most of the federal government. if you want to bury your head in the sand, believe in easter bunnies and santa clause and the FDA then bless you, wonder off into the woods blind.
you can’t trust Vets, you can’t trust the government, you can’t trust pet food companies. RAW is the ONLY way to feed.
Honestly, the claim that this page is scientific is laughable. You’d get an honest F from a highschool teacher when it comes to citations. Honestly, learn how to post credible links and not just “here’s my page again”
Fluoride is pure poison..it comes from China as a hazardous waste. and we do need detox…This whole page and comments are a cluster F%%%…
If you really are a vet, which I doubt SERIOUSLY!! You should do your own study instead of pontificating about a product you’ve only read about. Proof is in the pudding, buddy. And science is experience, of which you’ve said nothing about. You’re the snake ? oil!
Science my ass!
You would make a good democrat. Your innuendoes are sickening.
Time for Some Anger Management
The only quackery that is happening here is this BS article some angry person who goes by the vet school books aka purina guide on how to keep your animal alive..(or dead id say) This article made my blood boil 1 because Dr.Karen Becker has more balls than any of you tiny brainwashed humans coming out of vetschool… if your veterinarian is anything like this quak continue searching for another…I LEGIT HATE u whoever u are.
Why dont you shut the F up , people do put negative posts on websites , your problem is you believe everything the vet tells you , your Probably a vet anyways
So go fuck yourself skeptvet. You miserable pessimistic piece of shit. Not helpful. Just shut your face. Zip it. Sew it up. Shovel dirt in your face and your mouth. No one cares for your opinion. You probably just like accepting defeat and yeah like you’ve live enough etc etc.
You should be ashamed for writing this article. You make me sick to my stomach and I hope one day you learn your lesson. I doubt you will though, people like you are what is wrong with the world.
And your answer .. is Scotch .. even jokingly that just tells why your brain cells are deteriorated.. and you are obviously a closed minded, stubborn know it all Democrat . One day when you discover the truth about the same stances you ridicule I hope you don’t have a melt down .
These people who wrote this damn article are clueless!!!
This critique comes across as pathetic, petty, and desperate.
Wow, do you really believe that? There are literally hundreds of studies, if not thousands, from around the world that say otherwise. Do your research you lazy quack.
you are trash bich fuck you ass hole
Clown
Unfortunately your attitude in common with most vets I have had the misfortune to encounter over 40 years… which is always an unpleasant experience…because of the self serving attitude of the veterinary know all, the lack of social abilities, the appalling system which makes animals suffer by extensive waits and the desperate need to make as much money as possible based on fear.
You are PRECISELY what is wrong with today’s Veterinary Medicine, you should be ashamed
This skeptic is an evil arch enemy of the cure that costs little compared to the vet pharma!!! Ive seen this work!!! SHAME ON THIS SKEPTIC FOR WITHHOLDING CURES FROM ANIMALS AND PEOPLE!!!
What an evil, hateful, fake person you are. How do you live with yourself? Shame on you for lying to and misleading people who are trying to give their beloved pets the best care. What’s your motivation? Do you feel like a super special big shot now? Or money, I bet. Who’s paying you, big pharma, dry dog food companies? You disgust me.
Based on this arical I will not refer to skeptvet ever again for anything. My opinion of Skeptvet is this: Skeptvet is a worthless source. I hope the writters for this site don’t have animals. They surley don’t know a thing about them.
God skeptvet, you are Sincerely an idiot, without a clue…like most vets your a stubborn Ass,
Skeptvet please take your “science” and shove it up to your a#$$%%. Not all science works all the time. Some of my patients have been saved with a combination of holistic/natural and western medicine. So please make us all a favor and stfu.
My guess is that you are a bored, unemployed and clearly disgruntled, dog walker perhaps?
You’ve got that manipulation tactic down pat!! If you weren’thiding behind some pseudonym, I’d report you to the Veterinary Licensing Board myself!! And I sure as heck wouldn’t visit your practice with a flea as a pet. You’re awful!!
I am so glad you’re not my pets vet! Oh wait, we don’t even know if you are a real vet! This blog smells like snake oil! Happy trails Mr. Mystery Vet (what does that matter who you are).
You, Mr. Author of this article, are full of crap. You are an asshole writing this article to hurt this small company. I do not care about studies – proof is in miraculous results. I do not care about your B.S. You need to pull your head out of the sand & stop writing false propaganda.
It has been proven that vaccine cause disease. But you are one of these idiot who will trust his alternative doctor (who just don’t know any fuck about all the FDA cartel) Wake the fuck up before saying that and go read the full list of all doctors murdered by FDA because they found 100% cancer/HIV cures. You, kind of person like you make me angry as i can’t even believe how people can be sooo much idiot thinking that cancer cure didn’t exist, but still, we went to moon. Read the full story of FDA before saying something. Man you just can’t be serious ???? This is why i lost faith in humanity. Wow. I just can’t believe.
The Tone Police
Wow, you really look down to people who comment on your post and have a different views than your own. So rude.
I do not appreciate your verbiage referring to dr Jones. Very inappropriate and unprofessional. Shame on you skeptvet!
The skeptvet in my opinion is too negative and harsh….The manner skeptvet responds is in my opinion heartless.
Clearly no one will ever win an argument with Skeptvet because he ‘knows it all’ and enjoys patronising people who don’t agree with him – just like all the TV doctors and medics that seem to think that only what they say matters and the rest of us are clueless idiots, unable to think or research for ourselves
One of the most common topics over the lifetime of this blog has been treatments for osteoarthritis in dogs and cats. I’ve talked about pharmaceuticals, acupuncture, electromagnetic fields, laser, and other treatments, but the bulk of the articles have addressed the most popular over-the-counter (OTC) remedies for this condition, dietary supplements.
Supplements are ubiquitous, recommended by vets and used by owners frequently despite scientific evidence that is inconclusive or that outright shows they don’t work. Over the time I have been covering this topic, science-based medicine has provided new tools for treating arthritis, such as the use of monoclonal antibodies to reduce pain and inflammation in dogs and cats. For most pets, non-steroidal anti-inflammatory medications (NSAIDs) also remain a safe and effective treatment. There are also promising approaches, such as CBD and physical therapy, that have some encouraging supportive evidence, though more research is certainly needed for these. Despite this, pet owners, and even vets, have a tendency to stick with outdated OTC remedies that are unproven or even clearly ineffective.
The paragon for this is glucosamine/chondroitin. I wrote about the poor evidence supporting use of this supplement in arthritis pets in the very first month of this blog, June, 2009. At that time, I stated-
There is virtually no good quality research on the use of glucosamine and chondroitin in veterinary patients. The best study so far, done in dogs, found a combination of these agents to be of no benefit for patients with osteoarthritis. Further research in animals with osteoarthritis is warranted, but at this time the evidence does not support the use of glucosamine and chondroitin in these patients.
Since then, the negative evidence has piled up, in humans and in animals. My most recent summary in 2020 concluded-
The failure to find consistent and compelling evidence of clinically meaningful benefits after decades of extensive research strongly suggests such benefits are negligible or nonexistent.
Despite the seemingly minimal impact of such consistently negative findings on pet owner behavior, I feel obliged to continue to review the evidence and encourage both vets and owners to use therapies with real evidence of safety and benefit whenever possible. A recent systematic review (the highest level of evidence available) has once again looked at glucosamine, along with a host of other diets and dietary supplements for arthritis in dogs and cats, and hopefully their findings will shift the zeitgeist a bit on how we manage this condition.
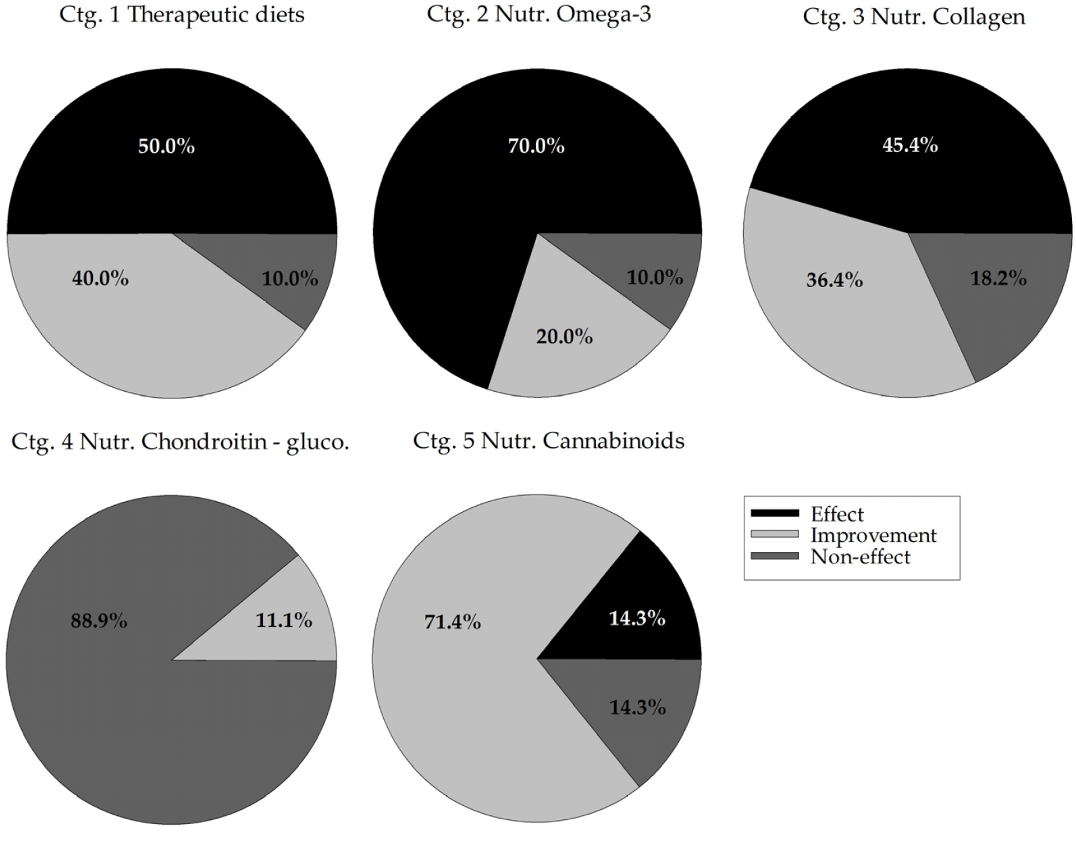
The figure below illustrates the quality of evidence for five categories of potential therapies. The proportion of studies showing the highest level of evidence, an effect compared with a placebo (Effect), an intermediate level of support, improvement over time without such a comparison (Improvement), or no effect at all (Non-effect) are shown.
The authors also evaluated the number and methodological quality of the research showing these effects and provided conclusions on each intervention. Here are those conclusions-
This meta-analysis supports the use of omega-3 supplementation for the management of canine and feline OA.
The results of this meta-analysis [for cannabis] are promising, but further investigation is needed to determine the efficacy, doses, formulations and combinations recommended for the treatment of canine OA pain. Further studies will also be necessary to conclude on the use of cannabinoids in cats since none have been carried out to this day.
It, therefore, appears impossible to rule, at the present time, on an indication for collagen in canine OA based on the results of this meta-analysis.
Like these previous reviews, the results of the present meta-analysis led to the conclusion that chondroitin-glucosamine nutraceuticals should not be prescribed in canine or feline OA.
All the other nutraceuticals evaluated did not present sufficient evidence of efficacy to decide on their indication.
I am not naïve enough to imagine that this will lead to a widespread abandonment of glucosamine, but I hope that the consistent buildup of evidence over decades showing that this is an ineffective treatment, and the active recommendations against it by experts in both human and veterinary medicine, will at least discourage the substitution of this failed approach for treatments with much better evidence for real effects.
I recently did this interview with the VIN News Service regarding the VIN Veritas Award and my work as a skeptic and advocate for science. We had a great chat about the start of SkeptVet and the critical need for active science communication and advocacy. And there’s a cute picture of my dog!
]WHAT IS AGING? How we define aging depends on our goals and our frame of reference. From the biomedical perspective of the veterinary clinician, the important elements are:
The passage of time
Deleterious physiologic and functional changes at the molecular, cellular, tissue, and organismal levels
A progressive increase in the risk of the three Ds
Disability
Disease
Death
As dogs age, they lose robustness (the ability to maintain a state of baseline or optimal physiologic function in the face of external stressors) and resilience (the ability to return to this state
following perturbations caused by such stressors).1 This leads to frailty and the development of many age-associated diseases which seem superficially unrelated but which are actually all consequences of the same underlying mechanisms of aging.
IS AGING A DISEASE? Because aging is a universal phenomenon, at least in mammals, and because historically there have been no effective interventions to slow or stop the aging process per se, only treatments to mitigate the clinical consequences, aging is widely seen as natural, inevitable, and immutable. However, decades of foundational research in laboratory model species, and more limited recent studies in humans and companion dogs, suggest that the core mechanisms of aging can be altered in a way that may prevent the health consequences of aging.2,3 Much debate has focused on the semantic issue of whether or not something natural and ubiquitous but also responsible for illness and death should be labeled a disease.4 There is not yet any consensus resolution to this debate.
A pragmatic approach that avoids this semantic debate is to view aging is the most important modifiable risk factor for disease in companion dogs. This is a familiar concept to veterinarians. Obesity, for example, is a risk factor for multiple specific diseases which increases the overall risk of mortality.5 Focusing on reducing this risk by targeting obesity, rather than waiting for the clinical consequences to develop and then managing each independently is a well-established practice in preventative medicine.
Age-associated changes are responsible for most of the health problems of adult dogs, and there are plausible hypotheses suggesting therapies that could directly target aging and so prevent these problems. The focus of geroscience (the study of the fundamental mechanisms of aging) is to identify these targets and therapies so the field of geriatrics (the clinical management of the aged) can move away from the reactive practice of treating the clinical consequences of aging as they arise and towards a preventative approach of delaying and preventing these consequences by modifying the fundamental processes of aging.
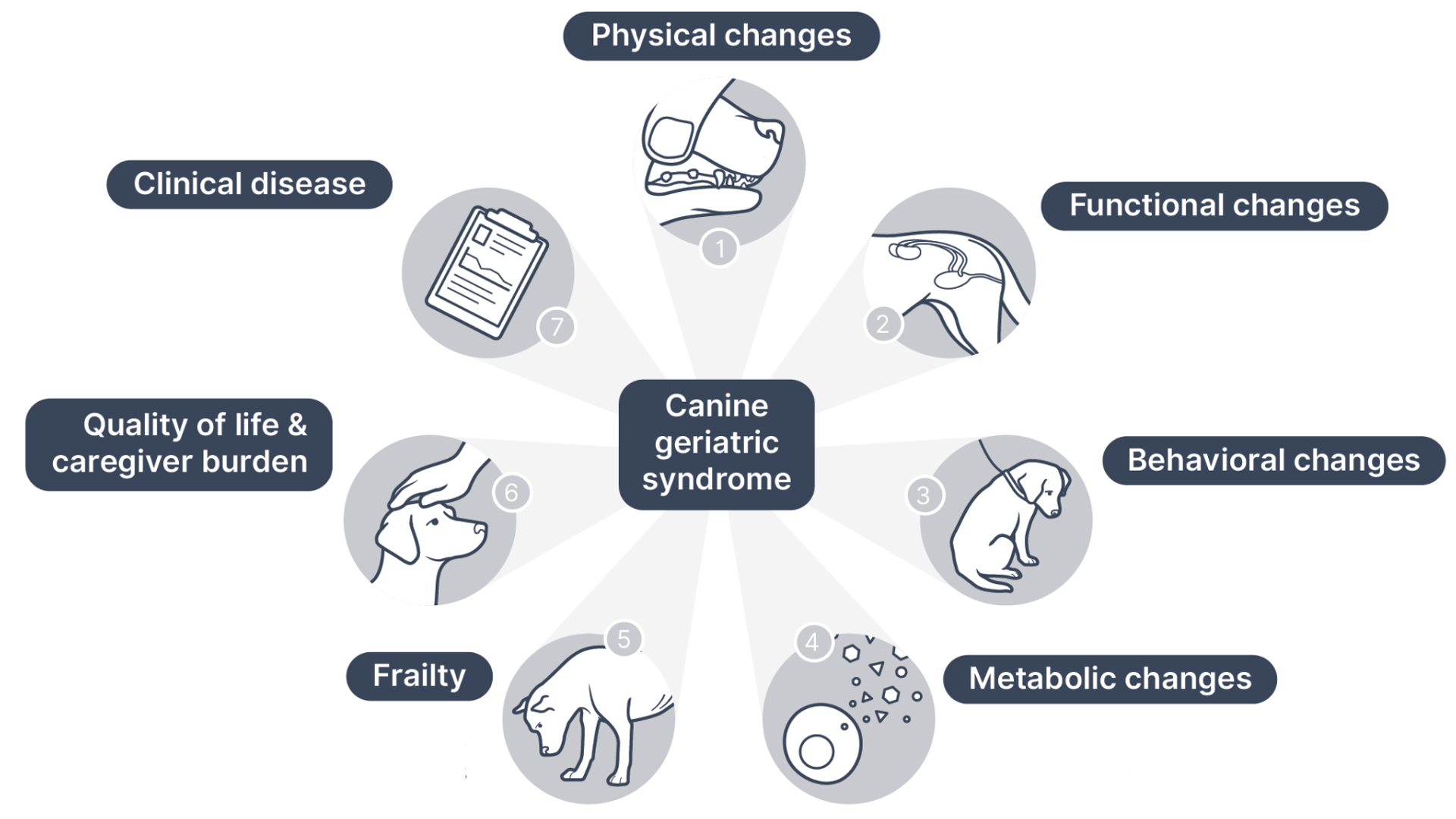
CANINE GERIATRIC SYNDROME Regardless of whether one chooses to think of aging as a disease, it is useful to characterize and measure the key elements of canine aging process, including the underlying mechanisms and the clinical phenotype. Canine Geriatric Syndrome (CGS) is both a conceptual framework to organize canine geroscience research and also a potential clinical assessment tool to help determine biological age and predict health outcomes in aging dogs. Figure 1 illustrates the components of CGS.
The fundamental mechanisms of aging, from the cellular and molecular level to the level of tissues and organs, generate a phenotype that includes physical, function, behavioral and metabolic changes. These culminate in frailty, which dimmish quality of life, burden human caregivers, and eventually lead to the key negative health outcomes: disability, disease, and death. Currently, this syndrome serves primarily as a scaffold focusing research to better understand the causes and manifestations of canine aging. Eventually, clinical assessment of the syndrome will be possible, leading to a diagnosis of CGS that quantifies the biological age of individuals, predicts morbidity and mortality, and guides clinical intervention.
HOW DO DOGS AGE? The cellular and molecular processes associated with aging, and the tissue dysfunction and ultimate health problems that result from these processes, are complex and multifactorial. Research in laboratory species, and in humans and our canine companions, has elucidated many of these mechanisms, and our understanding of them is growing rapidly. Typical changes include diminished stem cell number and function, declining mitochondrial number and function, accumulation of aberrant and dysfunctional proteins, and many others.1,6–8
Despite the complexity of aging, it is ultimately just biology, a collection of physiologic processes that can be understood and manipulated like any other. There is a vibrant field of canine geroscience research investigating the processes of aging and potential targets for intervention to extend healthspan and lifespan.
Aging manifests in many visible physical changes, from greying of the coat to lenticular sclerosis and loss of lean body mass. Functional changes include decreased mobility and diminished hearing and vision. Behaviorally, old dogs are often less active, less social, and more prone to anxiety and confusion, with many eventually developing canine cognitive dysfunction, a brain disorder similar in many ways to Alzheimer’s Disease in humans.
WHEN IS A DOG “OLD”? The old canard that every year in a dog’s life is equivalent to seven years for a human is a misleading oversimplification. Dogs age more rapidly than humans at the beginning and end of their life cycles, but the overall lifespan trajectory is quite similar.9 Large and small dogs often age quite differently as well, so the designation of geriatric status may be appropriate much earlier for some breeds than others. In terms of chronological age, or simply the time a dog has been alive, one has to consider size, breed, and individual characteristics. For practical purposes, this approximation is at least useful for triggering more intensive monitoring and investigation of clinical complaints, but it is merely a very rough guide to when we might call a dog “old:”
Small (under 20 lbs) > 12 years
Medium (20-50 lbs) > 10 years
Large (over 50 lbs) > 8 years
More important than chronological age, however, is biological age, defined as the degree to which aging has impacted the robustness, resilience, and state of health and function in an individual as measured by physical, functional, and biomarker assessment.1 We do not yet have reliable tools for measuring biological age, but many are being developed and tested, and ultimately this will be a much more accurate way to predict the age-associated risk of the three Ds (disability, disease, and death) than chronological age.
AGE-ASSOCIATED DISEASES AND CLINICAL PROBLEMS Most categories of disease become more common in older dogs, including neoplasia, degenerative musculoskeletal diseases (e.g. osteoarthritis and sarcopenia), cardiac disease (e.g. myxomatous mitral valve disease and cardiomyopathy), chronic kidney disease, and others. Apart from congenital disorders, infections, and trauma, most of the significant diseases and causes of death dogs experience result from the progressive accumulation of cellular and tissue changes associated with aging.
Important clinical problems often develop which are not always associated with a specific diagnosis of disease. Loss of mobility, pain, sensory and cognitive decline, and many other such aging changes diminish quality of life, increase caregiver burden, and eventually lead to euthanasia. The common view of these as “natural” and inevitable part of the lifecycle impedes appropriate assessment and management of these conditions and delays necessary research to develop preventative interventions to extend healthspan.
A SYSTEMATIC APPROACH TO ASSESSMENT & MANAGEMENT OF GERIATRIC DOGS Once age-associated health problems do develop, we can best care for our patients with systematic, rational, evidence-based assessment and management. There are many tools that allow us to evaluate pain, impaired mobility, frailty, and other manifestations of canine aging, and these are not yet widely and consistently used. Many of the most common age-associated diseases, such as chronic kidney disease, cardiac disease, and many types of neoplasia, have been the focus of extensive research, and there are often clinical practice guidelines and other evidence-based tools to help support high-quality therapeutic management of these conditions.13–15 And finally, despite some significant limitations, the emerging discipline of hospice and palliative care is an important element in caring for those patients most severely affected by aging.16
ASSESSMENT AND MANAGEMENT TOOLS An important part of a systematic approach to geriatric dogs is consistent, objective assessment and management of age-related diseases and clinical problems. This is best accomplished with the regular use of validated clinical metrology instruments and reliance, when possible, on evidence-based clinical practice guidelines. There are many CMIs available to quantify pain, mobility, frailty, quality of life, and the burden of care on the owners of geriatric dogs. Repeated use of these allows detection of changes over time, better evaluation of the effectiveness of therapies than unaided observation, and better communication with owners to facilitate decision making.
There are also numerous clinical practice guidelines available to support management of the most common age-associated problems and diseases. While some are more rigorous and evidence-based than others, all offer rational and systematic approaches that can help clinicians make comprehensive treatment and management plans.
PITFALLS IN CANINE GERIATRICS A systematic approach to geriatric medicine encourages proactive identification of disease and clinical problems and using the best available evidence to guide diagnostic and treatment interventions. Too often, clinical signs of frailty and disease are dismissed as “just slowing down” or “normal aging” rather than appropriately assessed, monitored, and managed. In the future, proactive and systematic detection of such signs will be a critical element in the determination of biological age and the decision to employ therapies targeting aging directly.
References
1. McKenzie BA, Chen FL, Gruen ME, Olby NJ. Canine Geriatric Syndrome: A Framework for Advancing Research in Veterinary Geroscience. Front Vet Sci. 2022;0:462. doi:10.3389/FVETS.2022.853743
2. Campisi J, Kapahi P, Lithgow GJ, Melov S, Newman JC, Verdin E. From discoveries in ageing research to therapeutics for healthy ageing. Nat 2019 5717764. 2019;571(7764):183-192. doi:10.1038/s41586-019-1365-2
3. Lawler DF, Evans RH, Larson BT, Spitznagel EL, Ellersieck MR, Kealy RD. Influence of lifetime food restriction on causes, time, and predictors of death in dogs. J Am Vet Med Assoc. 2005;226(2):225-231. doi:10.2460/javma.2005.226.225
4. McKenzie BA. Is Aging a Disease? DVM360. 2022;53(3):25.
5. Salt C, Morris PJ, Wilson D, Lund EM, German AJ. Association between life span and body condition in neutered client-owned dogs. J Vet Intern Med. 2019;33(1):89-99. doi:10.1111/JVIM.15367
6. López-Otín C, Blasco MA, Partridge L, Serrano M, Kroemer G. The hallmarks of aging. Cell. 2013;153(6):1194-1217. doi:10.1016/j.cell.2013.05.039
7. Sándor S, Kubinyi E. Genetic Pathways of Aging and Their Relevance in the Dog as a Natural Model of Human Aging. Front Genet. 2019;10:948. doi:10.3389/fgene.2019.00948
8. McKenzie BA. Comparative veterinary geroscience: mechanism of molecular, cellular, and tissue aging in humans, laboratory animal models, and companion dogs and cats. Am J Vet Res. 2022;83(6). doi:10.2460/AJVR.22.02.0027
9. Wang T, Ma J, Hogan AN, et al. Quantitative Translation of Dog-to-Human Aging by Conserved Remodeling of the DNA Methylome. Cell Syst. 2020;11(2):176-185.e6. doi:10.1016/j.cels.2020.06.006
10. Salt C, Morris PJ, Wilson D, Lund EM, German AJ. Association between life span and body condition in neutered client-owned dogs. J Vet Intern Med. 2019;33(1):89-99. doi:10.1111/JVIM.15367
11. McKenzie BA. What does the evidence say about feline fitness and dog aerobics? Vet Pract News. Published online January 2022:25-26.
12. Urfer SR, Wang M, Yang M, Lund EM, Lefebvre SL. Risk Factors Associated with Lifespan in Pet Dogs Evaluated in Primary Care Veterinary Hospitals. J Am Anim Hosp Assoc. 2019;55(3):130-137. doi:10.5326/JAAHA-MS-6763
13. (IRIS) IRIS. Treatment Recommendations for CKD in Dogs.; 2019.
14. Keene BW, Atkins CE, Bonagura JD, et al. ACVIM consensus guidelines for the diagnosis and treatment of myxomatous mitral valve disease in dogs. J Vet Intern Med. 2019;33(3):1127-1140. doi:10.1111/jvim.15488
15. Biller B, Patel M, Smith D, Bryan C. 2016 AAHA Oncology Guidelines for Dogs and Cats*. J Am Anim Hosp Assoc. 2016;52:181-204. doi:10.5326/JAAHA-MS-6570
16. Bishop G, Cooney K, Cox S, et al. 2016 AAHA/IAAHPC End-of-Life Care Guidelines. J Am Anim Hosp Assoc. 2016;52(6):341-356. doi:10.5326/JAAHA-MS-6637)
SUMMARY INCLUDING 5 KEY “TAKE HOME” POINTS
Aging is not an inevitable and immutable fact of life. It is a modifiable risk factor for the most causes of disability, disease, and death in adult dogs.
Canine Geriatric Syndrome describes the physical, function, behavioral, and metabolic changes that occur in aging dogs that lead to clinical disease, frailty, diminished quality of life, and a significant caregiver burden on dog owners.
Aging is just biology! The cellular, molecular, and tissue changes that occur, and that lead to Canine Geriatric Syndrome, are complex but comprehensible. The better we understand these changes, the better we can intervene to mitigate them.
A systematic, evidence-based approach to assessment and management of diseases and clinical problems in geriatric dogs, supported by validated clinical metrology instruments and clinical practice guidelines, is a more efficient, comprehensive, and effective strategy for high-quality patient care.
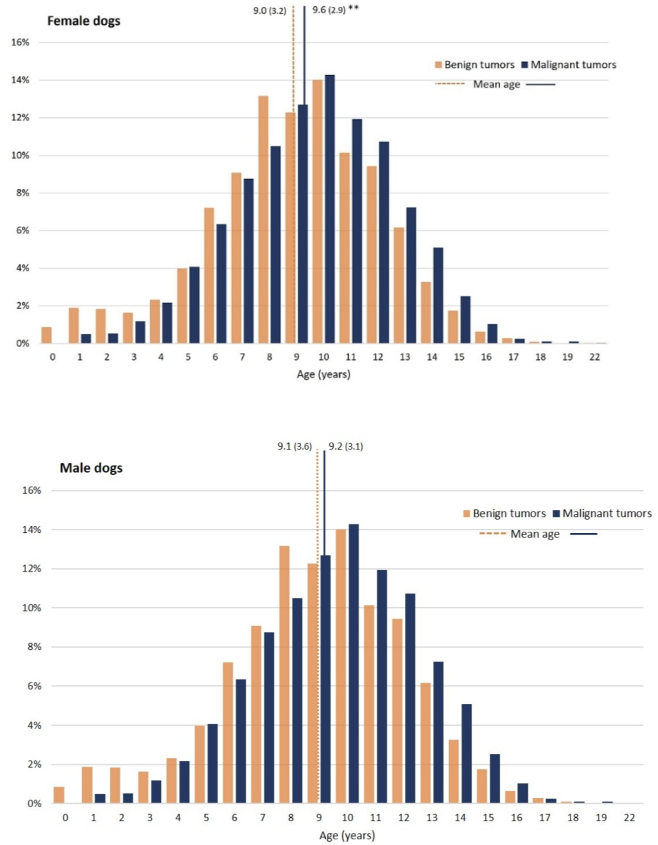
Cancer is one of the most dreaded diseases pet owners and veterinarians must contend with. While data are frustratingly sparse, there is no doubt that cancer is common in dogs, with estimates ranging from 25% to 40% of dogs likely to have a cancer diagnosis at some time in their life.
That time, of course, is nearly always in middle age or later. Cancer is a classic disease of aging. While young dogs, and humans, do sometimes get cancer, the vast majority of cases occur in older individuals. These charts show the frequency of benign tumors and cancers in male and female dogs by age. Cancer is quite rare until about 6-7 years, and then it rapidly becomes much more common. (Interestingly, cancer rates actually decrease in the very oldest dogs. Some of this is just a function of there being few dogs that reach this age at all, but there appear to also be some biological reasons why individuals who reach extreme old age are actually less likely to get cancer than they were when they were younger [e.g.here and here]).
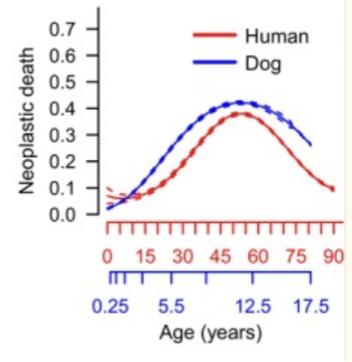
Comparison of cancer deaths in humans and dogs show a nearly identical pattern, with a dramatic increase in cancer risk around the period that can loosely be considered “middle-aged,” and then some decline in extremely old populations.
Of course, cancer is not a single disease, but a general type of disease that can manifest in many different places and ways. Because of this variety, there is no single “cause” of cancer, nor likely to be any single “cure.” However, a limited set of things have to happen for cancer to develop and cause illness. These include-
Spontaneous or inherited mutations in genes that support uncontrolled cell growth or inhibit the body’s natural defenses against it
Changes in the regulation of gene activity (aka epigenetic changes)
A permissive cellular environment that allows uncontrolled cell growth and spread of abnormal cells
Most often, multiple things have to go wrong for cancer to develop and progress to cause actual disease. Several layers of controls on cell growth must fail, and multiple mechanisms for identifying and eliminating abnormal cells must malfunction. Events that could lead to cancer are occurring in all of us all the time, but without the “perfect storm” of multiple failures, we never know it. This perfect storm becomes more likely as we age because of the accumulation of failures in the systems that prevent the development and survival of cancer cells.
Because carcinogenesis (the development of cancer) is so complex, dangerous oversimplifications are common. It is undeniable, for example, that some environmental risk factors can increase the chances of cancer. Smoking is one of the clearest examples, leading to a dramatic increase in risk of several types of cancer. However, even in this case, it is mistakenly simplistic to say that “smoking causes cancer” without acknowledging that this is a crude shorthand for “smoking increases the risk of cancer.”
Most people who smoke start doing so in their teens of twenties, yet most don’t develop tobacco-associated cancers until they are in their fifties or sixties. Some heavy smokers never get cancer at all. There is more to the story than just this one risk factor. Age, genetics, and other environmental factors also play a role.
While it is absolutely true that smoking increases the risk of developing cancer, and no one should ever do it, an overly simplistic view about how this works has become part of an unfortunate tendency to overestimate the importance of “toxins” and “chemicals” and visible risk factors that are perceived as “unnatural” while ignoring the equal or greater importance of unavoidable factors such as the passage of time or genetic predisposition. The laudable desire to minimize environmental risk factors becomes the extreme paranoia that sees all human products and activities as “unnatural,” and therefore harmful, and views cancer as a consequence of poor choices rather than an inherent risk of being alive.
I have discussed this extreme view, and its use to peddle quack remedies and dubious lifestyle advice before (see my post The Truth Behind “The Truth about Pet Cancer” and my review of The Forever Dog). The idea that we and our dogs are living in a “toxic” world that is causing rampant cancer, and that we could avoid it if we would just feed the “right” foods or supplements and avoid the “wrong” diets, medicine, vaccines, or whatever, is simplistic nonsense.
Fear sells, and cancer is legitimately terrifying. Sadly, proponents of unscientific strategies for preventing cancer will often use our fear as a tool, claiming that there is an “epidemic” of cancer, in dogs and humans, and that we are more at risk than ever before. This is almost certainly untrue in humans. The occurrence of some cancers is increasing (e.g. breast cancer in women) while other cancers are becoming less common (e.g. small cell lung cancer in men, thanks to a decline in the popularity of smoking, and cervical cancer, thanks to the HPV vaccine). Overall, the occurrence of cancer seems to be declining, and the death rates from cancer are absolutely improving, due to constantly improving prevention, detection, and treatment. Unfortunately, the data are too limited to support any strong conclusion either way in dogs.
While the concept of a “cancer epidemic” is hyperbole, it is fair to ask if cancer is more common today than it was in the past, even if we do not buy into fairytales about the past as a health “Golden Age” in which humans and dogs lived longer, healthier lives (exactly the opposite of the truth). There is, as it turns out, some reason to believe that cancer is more common in both species than it was in the past.
Again, the situation is complex, and the types of cancer seen have changed over time due to changes in various risk factors. Stomach cancer in humans, for example, declined by 90% during the twentieth century, as refrigeration replaced salting and smoking as a means of preserving foods. This is a clear example that the myth of a healthier pre-industrial lifestyle is nonsense.
However, many other types of cancer did become much more common during the twentieth century in people. This is often attributed to an increase in environmental risk factors, including purported “toxins.” While this is true in some cases (smoking and some industrial pollutants being clear examples), it overlooks one of the most important reasons why cancer in humans increased during this time, and also a likely reason why cancer probably increased in dogs as well. The simple fact that people, and probably dogs, are living longer.
Cancer is an age-associated disease, and the longer individuals live, the more likely they are to develop it. A population with more older people, or dogs, is going to have more cases of cancer. And there is no doubt that human populations throughout the world are getting older as people are living longer.
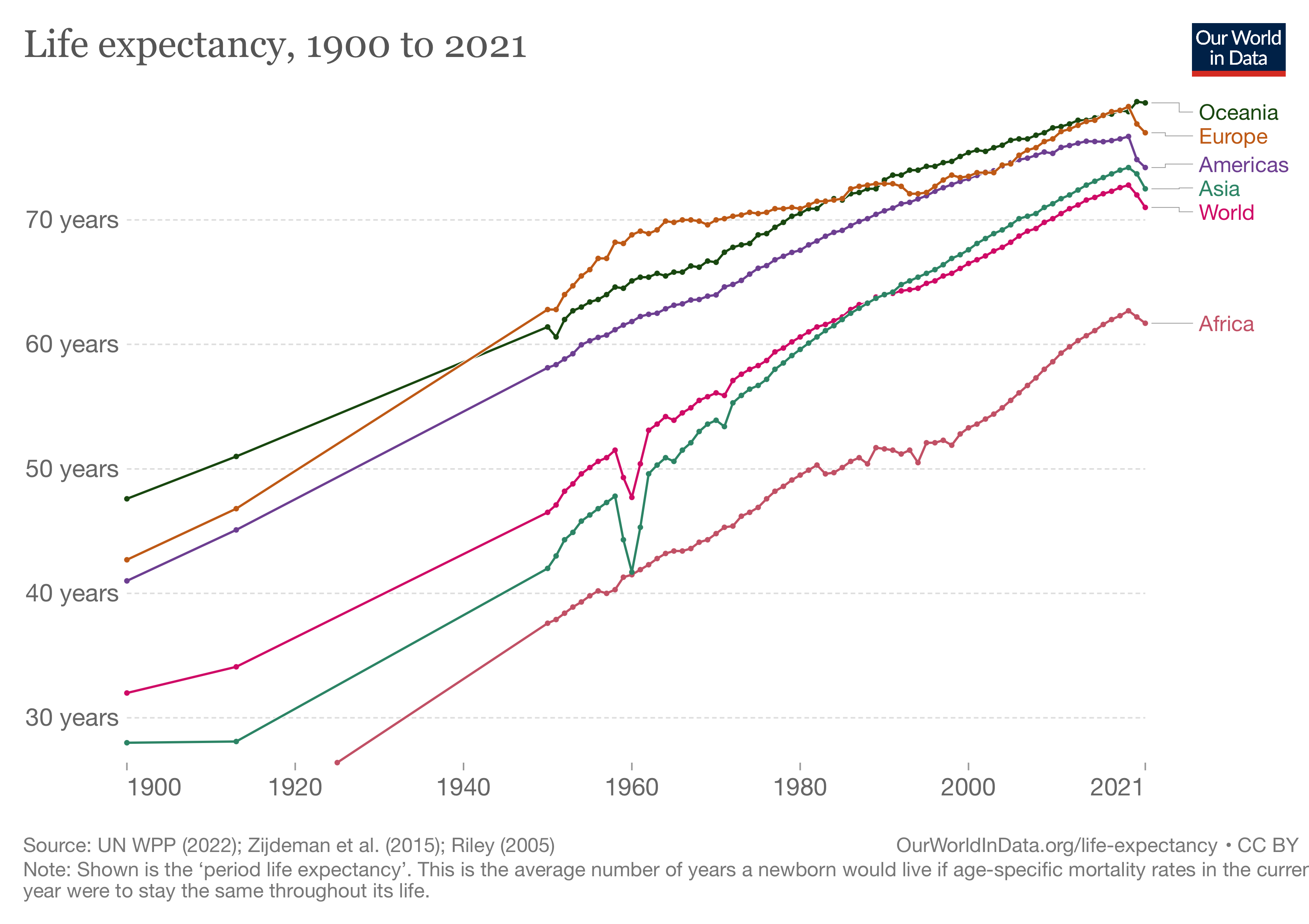
Human life expectancy has increased dramatically, thanks to the fruits of scientific discovery. Food production, nutrition, vaccination and healthcare, sanitation, accident prevention, and many other changes have reduced or eliminated numerous causes of death, especially in children, and led to a population with a much higher proportion of old people.
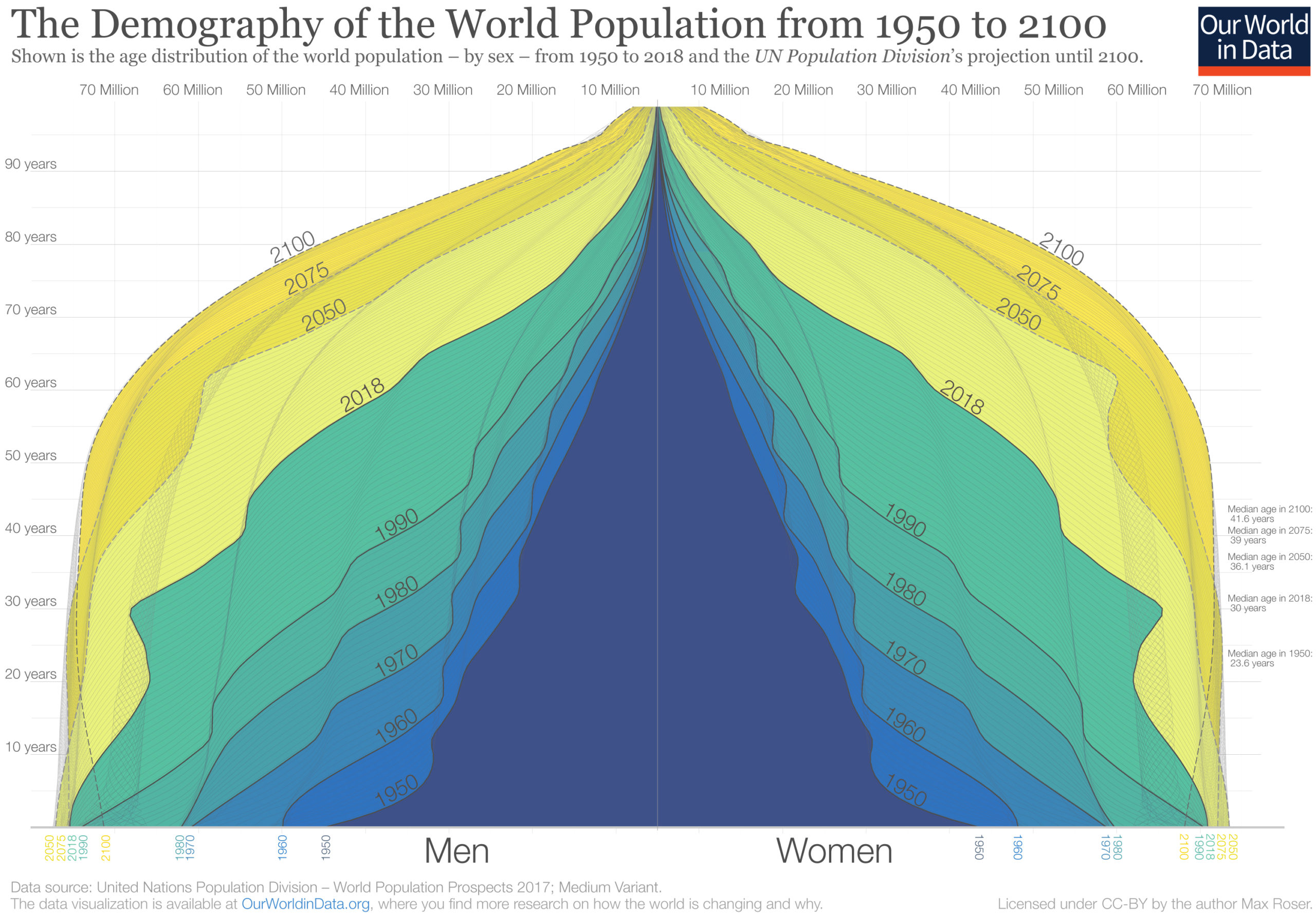
The chart below is a little unusual, but it shows the proportion of the world’s population in each age group for the years 1950-2018 (and then estimates from 2018 to 2100). Even in this short period, from the middle of the twentieth century, the proportion of people in middle-age and older has exploded.
As I’ve discussed before, it seems likely that owned dogs have experienced a similar increase in lifespan, and in the proportion of old dogs in the population, but there isn’t much hard data available.
Apart from the likely increase in cancer rates due to an increase in the number of old individuals, a recent paper has proposed another possible explanation. Not only are humans, and probably dogs, living longer, but we have extended our lifespan dramatically over such a short time that evolution has been unable to adjust our biology to account for this, leaving us vulnerable to age-related diseases that some even longer-lived species are protected against.
It turns out that if a species occupies a niche that favors a longer life, and the lifespan of individuals in that species increases gradually over evolutionary time, then genetic adaptions develop which delay the onset of age-related diseases. Elephants, whales, sharks, parrots, and the unusually long-lived rodent known as the naked mole rat, all have long lifespans in nature, and they have all developed a variety of genetic mechanisms protecting them against cancer throughout their lifespan.
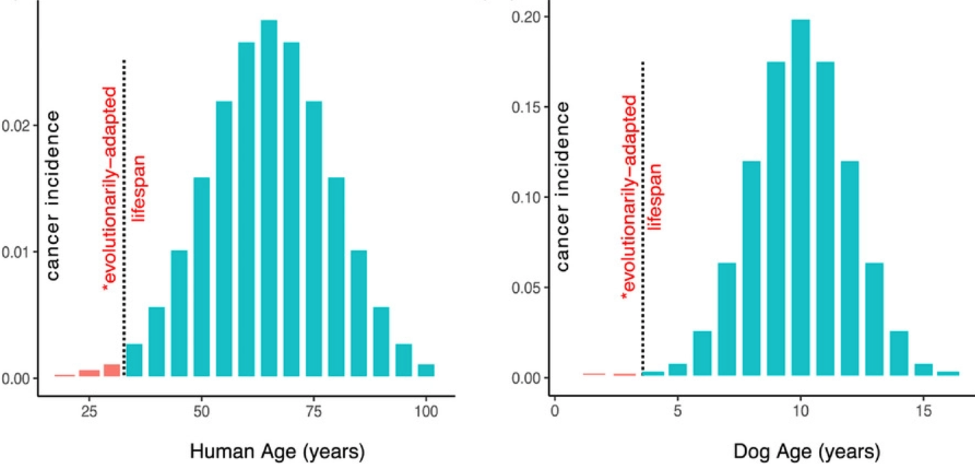
While humans are a relatively long-lived as mammals go, the “natural” life expectancy for most of our species’ history, prior to the development of science and science-based technologies, was about 30-40 years. This is as long as evolutionary mechanisms protecting against cancer would be expected to have developed to work since there was no evolutionary need for protection past the age when the large majority of people died.
This nature lifespan happens to line up quite neatly with the age at which cancer rates increase dramatically in humans today. Fewer than 5% of cancer cases occur in people under 35 years old, and fewer than 10% in people under 45. The vast majority of cancer occurs in humans older than the natural expected lifespan.
Similarly, wild and feral dogs tend to have a lifespan of less than 5 years. This is likely similar to the natural lifespan of dogs before modern pet ownership, with improvements in nutrition and medical care, became common. Owned dogs now routinely live at least 8-10 years in large breeds and commonly into their mid-to-late teens in smaller breeds. As in humans, fewer than 10% of canine cancer cases occur in dogs under 5 years of age. Most cases occur in dogs older than most dogs would have lived before the very recent past.
Evolution could not have provided protection against cancer throughout the lifespan in humans and dogs, as it has in elephants and sharks, because such changes require thousands to tens of thousands of years and many generations to develop. Such protections only exist through the expected natural lifespan, which was the same for most of our species’ history and much shorter than our typical lifespan today.
The simple way of putting this idea is that we and our dogs are victims of our success! We have extended our lifespans “unnaturally” far faster than evolution could have done, so there has been no time to develop the kind of protections against age-related diseases such as cancer that exist in species that naturally live a long time. As the authors of the paper explain it,
A major component of the elevated cancer risk seen in domestic dogs and in humans when compared to other animals is due to the shattering of the life-expectancy barrier that was evolutionarily determined: essentially “living longer than nature intended.”
The excess of cancers seen in modern dogs (and in humans), and the patterns of their association with age, would strongly suggest that there has been neither sufficient time nor selective pressure to allow for evolution of adaptive mechanisms to reduce the risk of cancer that comes with the creation of aged cellular environments, increased exposures, and the accumulation of somatic mutational events in these populations.
In dogs and humans, recent dramatic alterations in healthcare and social structures have allowed increasing numbers of individuals in both species to far exceed their species-adapted longevities (by two to four times) without allowing the time necessary for compensatory natural selection. In other words, the cancer-protective mechanisms that restrain risk at comparable levels to other species for their adapted lifespan are incapable of providing cancer protection over this recent, drastic, and widespread increase in longevity.
While this may not be the whole explanation for differences in cancer rates between species, it is a plausible hypothesis with reasonable support. The good news is that we may be able to compensate for the lack of evolved cancer protection in humans and dogs despite having dramatically extended our lifespan through a variety of strategies. Certainly, identifying and avoiding environmental risk factors should be part of this effort. But we cannot focus exclusively on the “toxic environment” view, because it is incomplete. Our understanding of the underlying mechanisms of aging has expanded dramatically, and these mechanisms provide many targets for lifestyle interventions and medications that can extend healthy lifespan and reduce age-associated diseases like cancer.
In one sense, technology and science have created the problem, though not in the way that shrill critics of modern life believe. We have defeated many causes of illness and death that afflicted us and our canine friends for millennia. This has left behind others that were never a threat when we all died young of the causes we have now tamed. But we can use the same processes of scientific discovery to understand the new threats and tame them as well, giving us and our dogs as much happy, healthy time together as possible!
I received some exciting news today. As always, I am very grateful to everyone who has been supportive of my advocacy and science communication work over the years and who has found it useful (that means all of you!!).
The VIN Veritas Award – from the Latin for truth – honors those who serve science and truth through courage and integrity.
This year, I’m pleased to announce another worthy recipient to join their ranks.
Brennen McKenzie, VMD, MS (Physiology and Behavioral Biology), MS (Epidemiology), is a small animal practitioner, instructor in evidence-based medicine, and author of the Skeptvet blog. Brennen has long been admired by colleagues for his dedication to promoting evidence-based veterinary medicine, and I am delighted that the 2022 VIN Veritas Award judges saw fit to honor his work.
EVIDENCE-BASED MEDICINE There are many characterizations of evidence-based medicine (EBM),1–3 but nearly all include the following core elements:
Explicit integration of controlled research evidence into clinical decision-making
Acknowledgement that some types of evidence are more reliable than others. This is frequently illustrated with hierarchical structures such as evidence pyramids, as in Figure 1.
Recognition that evidence generated by controlled scientific research is generally superior to anecdotal evidence and uncontrolled experience or observation.
A pragmatic acceptance that clinical decisions must be based on the best available evidence, regardless of the level, and should incorporate the judgement of the clinician and the goals and resources of key stakeholders (e.g. human patients or veterinary clients).
Figure 1. Hierarchy of evidence, from most available and least reliable at the bottom to most reliable and least available at the top.4
EBM is a powerful tool for improving patient care, reducing medical errors, compensating for cognitive biases and other sources of faulty decision-making, and meeting the ethical obligations of clinicians to provide the most effective possible treatment and to obtain true informed consent. The major limitations of EBM in veterinary medicine include the paucity of high-quality scientific evidence and a culture of reliance on anecdote and personal experience rather than controlled research evidence.
VETERINARY PALLIATIVE AND HOSPICE CARE The clinical practice guidelines of the International Association of Animal Hospice and Palliative Care (IAAHPC) define palliative care as “relieving or soothing the symptoms of a disease or disorder at any stage of an illness.”5 The American Animal Hospital Association (AAHA) End of Life Guidelines define it as “treatment that supports or improves the quality of life (QOL) for patients and caregivers by relieving suffering.”6 The focus is symptomatic treatment to relieve suffering and improve quality of life, regardless of whether the cause of suffering is a terminal or curable condition. This is, or should be, an integral part of the ordinary practice of veterinary medicine, not relevant only to end of life care.
Hospice, on the other hand, is specific to patients with terminal or incurable conditions, and it is less straightforward to define. According to the AAHA guidelines, it is “philosophy or program of care that addresses the physical, emotional, and social needs of animals in the advanced stages of a progressive, life-limiting illness or disability.”6
The IAAHPC does not provide a single definition, instead discussing the origins and various elements of animal hospice and how it is similar and different from human hospice care. These discussions include the following key concepts:5
Provide palliative care not only for the imminently dying, but also for patients for whom a cure is no longer possible and whose condition has become advanced, progressive, and incurable
Give patients and caregivers control, dignity, and comfort during the time they have remaining to live
Offer spiritual support to patients and accommodates beliefs about death and about afterlife as much as possible. It also provides spiritual and grief support for caregivers
Including hospice-supported natural death as well as euthanasia.
EBM APPLIED TO PALLIATIVE AND HOSPICE CARE Both the AAHA and IAAHPC guidelines, as well as most books and training materials for veterinary professionals dealing with hospice and palliative care, acknowledge the importance of EBM for these disciplines:
AAHA-6
Evidence-based support for specific recommendations has been cited whenever possible and appropriate
Because each case is different, veterinarians must base their decisions and actions on the best available scientific evidence, in conjunction with their own expertise, knowledge, and experience.
Evidence-based research to support this rapidly evolving field is also necessary.
IAAHPC-5
Applying insights and knowledge from bioethics will expedite the development of evidence-based best practices in these emerging fields.
The fields of animal hospice and palliative care are still in the early stages of development and these Guidelines will require revision as evidence-based knowledge advances.
However, organizations and experts in this field also acknowledge that there is a deficiency in the evidence base for many of the practices commonly recommended and employed and that personal experience and extrapolation from human medicine or basic science, both examples of very low-level evidence, form the support for many of the day-to-day interventions and techniques used. This is, of course, also true in most other disciplines within veterinary medicine.
The lack of strong evidence supporting the effectiveness of many practices in hospice and palliative care diminishes the quality of patient care. The history of human and veterinary medicine is rife with ineffective and even actively harmful treatments that were believed to be safe and effective and were widely used for long periods of time before scientific study demonstrated their deficiencies. From bloodletting and homeopathy to thalidomide and internal mammary artery ligation, therapies supported by personal experience and low-quality evidence have been failing patients for thousands of years.7,8
Perhaps a greater challenge to more evidence-based palliative and hospice care than the current lack of high-level evidence is the centrality of philosophical, ethical, and spiritual considerations in these fields. In human hospice, the goals of a hospice program, and the success of hospice and palliative care in any individual case, are inherently intertwined with the beliefs and values of the humans involved. This is an explicit feature of human hospice, where the spiritual beliefs of the human patient and family members are key drivers of the hospice plan for an individual.
Central tenets of the human hospice movement are predicated on contemporary cultural and religious beliefs. For example, a common guiding principle is that hospice care should never hasten death,9 and this is largely a response to general societal views about the sanctity of life and prohibitions on euthanasia, which are rooted in religious and spiritual belief systems.
The animal hospice movement recognizes that veterinary professionals operate in a different context. Our patients cannot express philosophical or spiritual beliefs, and it is debatable whether they are capable of entertaining such beliefs or whether non-human animal cognition encompasses concepts such as the meaning of life or the existence of an “afterlife” of some sort. Euthanasia is also universally legal and widely considered an appropriate choice for animals with impaired quality of life or incurable disease, which provides a very different possible endpoint for hospice care than is usually available for humans.5,6
However, the feelings and belief systems of our patients’ human caregivers are certainly relevant to the formulation and implementation of palliative and hospice care. Philosophical and emotional motivations for choosing natural death rather than euthanasia are likely a significant reason for seeking animal hospice care. The acceptance or rejection of specific treatments is also often informed by such beliefs, which sets limits on the options available to the veterinary team.
EBM is not readily applicable to most religious or ethical issues. When or whether it is acceptable to euthanize an individual animal or permit a natural death, for example, is not a question scientific evidence is well-suited to settle. And while scientific evidence is useful to inform our understanding of how animals experience pain and other forms of physical suffering, it cannot clearly answer existential questions about what meaning life may have to our patients or whether spiritual considerations are relevant to them. The complex ethical balancing of the interests of the patient as understood by the veterinary team and the understanding and interests of the patient’s human family relies more on the domains of ethics and philosophy than on medical scientific research.
Ethical and philosophical issues are relative to one’s particular world view, and this will vary significantly between groups and individuals. Because the community of veterinary professionals actively working in hospice and palliative care is relatively small, the practices and guidelines within the field are heavily influenced by the beliefs and perspectives of a limited number of individuals. This may make the principles and practices of the discipline less compatible with other points of view and could discourage some veterinary professionals or animal owners from providing or seeking palliative and hospice care or taking full advantage of its benefits. As the field grows, a broader range of perspectives may have a beneficial effect on the core principles and common practice.
There are, of course, many aspects of palliative and hospice care to which EBM can and should apply. The safety and efficacy of individual therapies, the most effective way to measure pain and other forms of physical discomfort and to assess the impact of therapies on these, and other important elements of effective palliative and hospice care do depend on accurate knowledge of the kind most effectively generated by controlled scientific research. While there are unique issues in hospice care that influence how we study such questions, there is no doubt that providing effective care requires that the veterinary team and the patients’ caregivers have an accurate understanding of the diseases, symptoms, and treatments involved.
One area that reflects the influence of belief systems and personal experience and the lack of strong EBM standards is the incorporation of so-called complementary and alternative therapies in hospice care. Despite the lack of high-quality evidence for the safety and efficacy of most of these interventions, and strong negative evidence against some, they are widely utilized in both human and animal hospice. Though not mentioned directly in the AAHA guidelines, such alternative practices are explicitly endorsed in the IAAHPC guidelines.5,6
The culture of alternative medicine emphasizes the primacy of personal experience over empirical scientific evidence in evaluating medical treatments, and the role of spiritual considerations in healthcare is often seen as critical.10 These views are also part of the culture of end-of-life care in both human and animal hospice. The training materials for the AAHA certification program in palliative and hospice care explicitly endorse therapies with questionable supporting evidence (e.g. herbal remedies and acupuncture) and those which are clearly only placebos (e.g. homeopathy and “energy” therapies) alongside science-based medical practices. This acceptance of dubious medical practices is likely encouraged by several features of the animal hospice culture and context:
The limited scientific evidence available to assess many common practices
The practical and ethical challenges of conducting high-quality research in patients with terminal conditions
The misperception that the risk of using therapies with inadequate evidence for safety and efficacy are lower in patients with terminal conditions than in patients we hope to cure
The influence of the personal beliefs and experiences of the relatively small number of individuals involved in developing and promoting animal hospice
The culture of the hospice movement, which emphasizes the primacy of individual experiences and beliefs and the centrality of spiritual considerations
TOWARDS MORE EVIDENCE-BASED PALLIATIVE AND HOSPICE CARE High-quality palliative and hospice care for veterinary patients is a critical part of a holistic approach to maximizing animal welfare throughout all life stages. The more evidence-based our treatments and practices are, the more confident we can be that these truly benefit our patients. While scientific research may not always be useful in informing all aspects of end-of-life care, such as supporting the spiritual needs of our clients, it is crucial to ensuring that we understand and meet the physical and behavioral needs of patients. Veterinary professionals and animal owners, like all humans, are easily misled by cognitive biases and placebo effects into inaccurate understandings of nature and the impact of our actions, and EBM can help us avoid such errors and provide the best possible care.11
Steps towards making animal hospice and palliative care more evidence based may include:
Continued recognition of the need for more and better-quality evidence to support palliative and hospice care practices
Improved understanding of the strengths and limitations of different types of evidence and the need to proportion our confidence in specific interventions or beliefs to the strength of the available evidence
Creativity and persistence in the generation of reliable scientific research evidence within the limitations of the palliative and hospice care context
Inclusion of a greater variety of perspectives and world views in establishing guidelines and training for hospice providers to maximize the value of these resources for the broadest possible population of veterinary professionals and animal caregivers
Willingness to change and abandon specific practices based on the best available evidence
REFERENCES
1. Sackett DL, Rosenberg WM, Gray JA, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312(7023):71-72. Accessed October 23, 2014. http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=2349778&tool=pmcentrez&rendertype=abstract
2. Mckenzie B. Evidence-based veterinary medicine: What is it and why does it matter? Equine Vet Educ. 2014;26(9). doi:10.1111/eve.12216
3. Cockroft P, Holmes M. Handbook of Evidence-Based Veterinary Medicine. (Cockcroft PD, Holmes MA, eds.). Blackwell Publishing Ltd; 2003. doi:10.1002/9780470690833
4. McKenzie B. Evidence-based Veterinary Medicine and Personal Bias. In: Ackerman L, ed. Pet-Specific Care for the Veterinary Team. John Wiley & Sons, Inc; 2021:39-42.
5. Shanan, A. August, K. Cooney, K. Hendrix, L. Mader, B. Pierce J. Animal Hospice and Palliative Care Guidelines.; 2009.
6. Bishop G, Cooney K, Cox S, et al. 2016 AAHA/IAAHPC End-of-Life Care Guidelines. J Am Anim Hosp Assoc. 2016;52(6):341-356. doi:10.5326/JAAHA-MS-6637)
7. McKenzie B. Placebos for Pets: The Truth About Alternative Medicine for Animals. Ockham Publishing; 2019.
8. Herrera-Perez D, Haslam A, Crain T, et al. A comprehensive review of randomized clinical trials in three medical journals reveals 396 medical reversals. Elife. 2019;8. doi:10.7554/eLife.45183
9. Finlay I. End-of-life care means exactly what it says: palliative care is about care at the end of life, not about ending life. Futur Healthc J. 2018;5(1):35. doi:10.7861/FUTUREHOSP.5-1-35
10. McKenzie BA. Is complementary and alternative medicine compatible with evidence-based medicine? J Am Vet Med Assoc. 2012;241(4). doi:10.2460/javma.241.4.421
11. McKenzie BA. Veterinary clinical decision-making: cognitive biases, external constraints, and strategies for improvement. J Am Vet Med Assoc. 2014;244(3):271-276. doi:10.2460/javma.244.3.271