One of my most popular, and controversial, topics to talk about at continuing education meetings is the evidence for abandoning practices that are deeply entrenched in routine veterinary practice. Vets are pretty good at adopting new things when evidence shows these might be worthwhile, often even when the evidence isn’t very good. But giving up things we are used to doing is much harder, even when the evidence is strong. Here are a few things vets might want to think about changing, and you might want to question if they are offered to you.
CHOOSING WISELY: THINGS TO STOP DOING IN YOUR PRACTICE (MAYBE)
THE JOY AND THE PAIN OF EVIDENCE-BASED MEDICINE
Veterinary medicine is a science-based profession. The philosophy and principles of science, and the data generated by scientific research, guide our clinical decision-making. The joyful side of this is that we get to watch new tests and treatments emerge during our career, and previously hopeless problems become treatable. The scourge of parvoviral enteritis has been dramatically diminished thanks to the development of a vaccine. The “incurable” malady of feline infectious peritonitis now seems to be beaten, at least in many cases, by new drugs. The first wave of monoclonal antibody therapies is just arriving, offering more treatment options for diverse problems such as osteoarthritis and atopic dermatitis.
The painful side of an evidence-based approach to practice is that we are often wrong. Not only does early and incomplete science sometimes lead us to the wrong conclusions, but as individuals we make even less reliable judgements based on personal experience and anecdote. What is worse, we develop strong emotional and ideological commitments to these judgements. Giving up a therapeutic practice that we believe in, that we were taught as youngsters and that we have since taught to others, that we “have seen work” in our own hands, is deeply unsettling. We don’t like to be wrong, and we don’t like things that challenge our understanding of the world, because that damages our self-image and makes the world seem less predictable and controllable.1,2
But the welfare of our patients is more important than our ego and our sense of security, and we have an obligation as practitioners of a science-based art to follow the evidence where it leads. This will inevitably mean abandoning beliefs and practices that are dear to us repeatedly throughout our careers. So, let’s square our shoulders, raise our chins, and rip off a few of those band aids today!
WHAT IS EVIDENCE?
Ok, before we do that, we should take a minute to consider what “evidence” is and how we decide when it is good enough to justify changing our practices.3 You’ve all seen some image like Fig. 1 before. The details are less important than the general point—not all evidence is equally reliable. The bottom of the pyramid contains the most available and accessible evidence– our experiences and opinions and those of others. The top of the pyramid is the smallest because it represents the evidence that’s the hardest to get– consistent findings across multiple, replicated, high-quality controlled research studies. So, we have lots of the least trustworthy evidence and only a little of the best stuff.
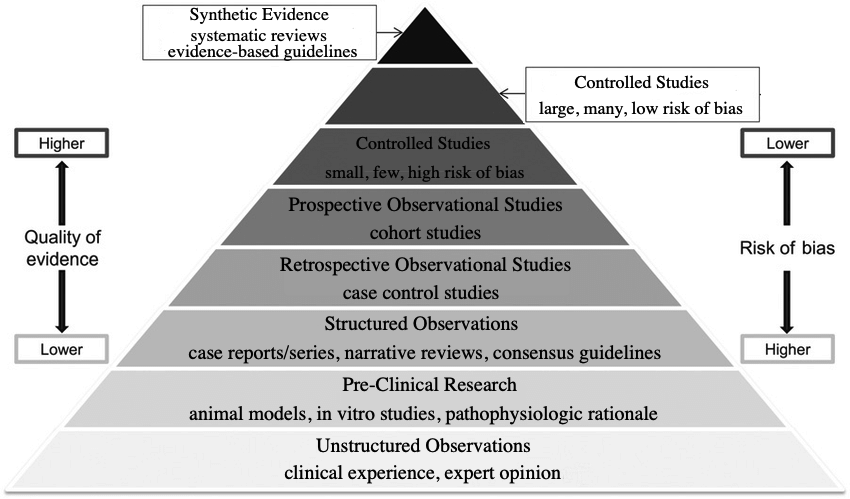
Figure 1. Types of evidence categorized by quality and risk of bias.
But the problem is even worse than that! The stuff at the bottom is by far the most psychologically compelling. Our brains are built to understand and trust our own experiences and the stories other people tell us about theirs. Data and numbers from research studies are a lot less satisfying and convincing.4 So we are most confident in the least reliable evidence and least likely to be moved by the evidence that history has shown us, again and again, is most likely to be correct. Bummer!
Science is not, of course, a perfect process. It is simply something humans have developed over a long period of trial and error to compensate for our inherent limitations. Scientific studies can be wrong and misleading, just like anecdotal evidence. Not every study is well-designed, properly conducted and analyzed, and not every study applies to all patient populations. There are a million reasons why scientific research evidence might lead us to the wrong conclusion. But there are ten million reasons why experience and anecdotes will mislead us!
The best we can do is recognize the problem and make an honest effort to remind ourselves often that what feels true may not be if it is based on uncontrolled experience and anecdote. If you find yourself saying, “But, I’ve seen it work!” take a deep breath and try to remind yourself that the proponents of blood-letting, magic healing rituals, and any therapy you believe is useless say exactly the same thing.
USES OF ANTIBIOTICS TO RECONSIDER
Treatment of Acute Diarrhea
The use of metronidazole as a treatment for acute diarrhea in dogs is a deeply entrenched practice that goes back decades. Various rationales have been proposed to support it, from treatment of potential bacterial causes, such as Clostridium, to anti-inflammatory mechanisms. Few general practice vets have not used this drug for this purpose, and there is abundant anecdotal evidence suggesting it is beneficial.
Unfortunately, there is also a growing body of research evidence showing little to no clinical benefit for most patients and some potential undesirable effects.5 At best, it might shorten the course of diarrhea by about a day. At worst, it can make symptoms worse, disrupt the microbiome in potentially harmful ways, and contribute to antibiotic resistance.
Given that the vast majority of dogs with idiopathic acute diarrhea will get better with time, these risks are hard to justify. Most humans don’t seek medical are or prescription drugs for mild, short-term diarrhea symptoms. The pressure to treat this condition in dogs has more to do with the inconvenience and anxiety it causes owners than the wellbeing of our patients. Although the risks seem small, it is difficult to justify them for a treatment that has mostly psychological benefits for vets and clients rather than medical benefits for patients.
It would be nice to have a clear alternative to offer here, but the reality is no research yet supports any specific treatment for acute, self-limiting diarrhea that is clearly effective and has negligible risks. Probiotics have not entirely lived up to their promise.6 Some evidence supports dietary change and fiber supplementation,7,8 but again most cases are self-limiting and likely to get better without any specific treatment.
Treatment of Upper Respiratory Infections
Like acute diarrhea, acute upper respiratory infections (URI) are often self-limiting in dogs and cats, and many have viral etiologies which will not respond to antibiotic treatment. There is limited controlled research comparing antibiotic use to alternatives, such as supportive care alone. Based on the clinical research that we do have, and also the basic science studies providing background on the causes and outcomes of feline and canine upper respiratory disease, expert consensus guidelines generally recommend limiting antibiotic use to cases with significant systemic symptoms (e.g. fever, lethargy) and evidence of bacterial involvement (e.g. mucopurulent discharge), or cases with chronic disease.9
Unfortunately, the lack of evidence for benefits from antibiotic treatment in most cases, and the potential for adverse effects and microbial resistance, vets still seem to often prescribe antibiotics unnecessarily for canine and feline respiratory infections.10,11 There is some indication, however, that awareness of, and adherence to, antibiotic use guidelines may be improving.12
Treatment of Urinary Tract Infections
Unlike upper respiratory disease, urinary tract symptoms often are caused by bacterial infection in dogs, and to a lesser extent in cats. These bacterial urinary tract infections (UTI) do sometimes require antibiotic treatment, though common practice in treating UTIs still often does not match current evidence-based guidelines.13
For one thing, just having bacteria in the urine does not a UTI make. Asymptomatic bacteriuria seems to be more common than previously recognized, occurring in from 1% to 13% of healthy dogs and cats, and at much higher rates in animals with immunosuppressive conditions or medications and other risk factors.13 In the absence of clinical symptoms, treatment with antibiotics does not permanently eliminate bacteriuria and appears to have no benefits for the patient. While evidence is somewhat limited in dogs and cats, it is clear that in humans prescribing antibiotics for subclinical bacteriuria raises the risk of adverse drug effects and antibiotic resistance without improving short-term or long-term outcomes for patients. This is true even if there is pyuria!13
Recommended treatment of symptomatic UTI confirmed by urine culture is also different from what many of us were taught long ago. Some of these cases may not require antibiotics at all. Humans with uncomplicated UTI are often treated symptomatically with NSAIDs, and the UTI often resolves by itself. This may be appropriate for veterinary patients too, though we do not yet have studies showing this.
Similarly, the recommended duration of treatment is 3-5 days, which is far shorter than the 7-10 day course many of us still prescribe. Even pyelonephritis is typically treated in humans with 7-10 days of antibiotics, and in the absence of better evidence experts currently recommend 10-14 days of treatment in dogs and cats, rather than the 4-6 weeks previously advised.13
One of the most common inappropriate uses of antibiotics for urinary tract signs is for young cats. In cats under about ten years of age hematuria, pollakiuria, and other symptoms of cystitis are far less likely to be caused by UTI (2%-19%) than in cats over 10 years of age (40-45%).14 Feline Interstitial Cystitis (FIC) is the most common cause of lower urinary tract symptoms, and of course antibiotics are not a useful or appropriate treatment for cats with FIC.15
Much of the antibiotic prescribing for urinary tract symptoms, as for gastrointestinal and respiratory symptoms, is driven by psychological factors: owner anxiety and demands for treatment, veterinarian anxiety about negative consequences to undertreating, and simple commission bias (the need to DO SOMETHING rather than wait for self-limiting problems to resolve on their own).4 Given that antibiotics are safe but not entirely benign, and that we are losing some effective treatments for serious infections to antimicrobial resistance, we should do what we can to resist the siren-song of antibiotic prescription above and beyond what is likely needed.
Perioperative Antibiotics
Speaking of anxiety, the prospect of a post-operative infection appears to haunt the nightmares of veterinarians, based on the rate at which many of us prescribe antibiotics for our surgical patients.
Available evidence suggests that surgical site infections are uncommon for most clean or clean-contaminated procedures (< 5%), and that giving antibiotics before or after surgery do nothing to prevent these. Even in cases with specific risk factors for infection, the most we should likely do is provide appropriate antibiotic coverage from 30-60 minutes before the procedure until 6 to 24 hours afterwards.16 There is no convincing rationale or evidence, from human or veterinary medicine, to support more extensive antibiotic use to prevent surgical site infections.
Veterinary dentistry is a special case of perioperative antibiotic use.17 Once again, extensive evidence in human medicine shows that bacteremia occurs with chewing, brushing, or flossing just as it does with dental procedures, and that antibiotics are not useful for routine prophylactic procedures. Only people at high risk of infective complications (those with implant foreign bodies, a history of certain cardiac diseases, or those who are immunosuppressed) are likely to benefit from antibiotics when having dental work.
There is a lot less data in veterinary patients, but the expert consensus is that antibiotics are rarely necessary for dentistry patients and are not justified except in those at high risk. Unfortunately, it isn’t clear who those patients are. Infective endocarditis is often suggested as a potential risk from dental procedures, but this appears to be extremely rare in dogs and cats. Overall, antibiotics are very unlikely to benefit the vast majority of veterinary dentistry patients, and their risks likely outweigh their benefits.17
Despite this, it appears that antibiotics are very commonly used in veterinary dentistry. In dogs and cats with established periodontal disease or requiring extractions (which describes most dentistry patients), antibiotic use appears to be very common, though use
varies widely between different veterinary facilities.18 More evidence and clearer guidelines would likely help reduce the overuse of antibiotics in veterinary dentistry.
USES OF ANALGESICS TO RECONSIDER
Tramadol
If ever there was a cautionary tale veterinarians should heed about an inappropriately used analgesic, it is the story of tramadol. A cheap and widely used opioid and serotonin agonist in human medicine,19 tramadol became a popular pain therapy in veterinary species despite some pretty significant warning signs that our enthusiasm for the drug was premature. Because it is a pro-drug that has to be converted to an active metabolite to have an effect, it should have been a red flag that this conversion is much less efficient in dogs than in humans.20,21
Nevertheless, it became popular for post-operative pain and for dogs with osteoarthritis. The use of tramadol was likely driven by anxiety about NSAIDs, which are the most extensive studies and most clearly effective oral analgesic for dogs and cats. Despite lots of data and a strong overall safety record,22 vets and pet owners seem especially worried about the potential risks of NSIADs and eager to adopt any alternative portrayed as safer, even when the data are scant.
Eventually, clinical studies accumulated showing that tramadol has marginal benefits over placebo for dogs.23 Caregiver placebo effect likely accounted for most of the appearance of benefits. And while tramadol has more of an analgesic effect in cats, due to more efficient conversion to the active metabolite, it also has pretty significant adverse effects in this species.24 Sadly, many dogs undoubtedly experienced inadequately treated acute and chronic pain, and some still do, because of our eagerness to accept a purported NSAID alternative and our willingness to believe anecdotal evidence for what we were hoping and expecting to see.
Gabapentin
The authors of the 2022 American Animal Hospital Association pain management guidelines for dogs and cats, at least, are trying to prevent history from repeating itself. They state, “Gabapentin has become the new tramadol, with widespread usage [despite] virtually no supporting data.”25
While there is good evidence in humans to support use of gabapentin for seizures and for some specific types of neuropathic pain (post-herpetic neuralgia and diabetic neuropathy), even most analgesic use in humans is without much supporting research evidence.26 In dogs and cats, there is limited evidence to support using gabapentin to reduce behavioral signs of stress, although it isn’t entirely clear if it reduces anxiety or is primarily a sedative. However, there is little reason to expect it to be of great benefit for acute or chronic pain. While more research needs to be done, it seems likely we have failed to learn our lesson from tramadol and are continuing down a similar road with this drug.
Mixing Lidocaine and Bupivicaine for Local Blocks
This is one of those ideas that sounds brilliant but is actually totally wrong!27 Some clinicians mix lidocaine and bupivacaine together with the idea that they will get “the best of both worlds–” the more rapid onset of lidocaine with the longer duration of bupivacaine. What actually happens is that you get the worst of both worlds!
The dilution of each drug leads to a lower concentration gradient, meaning less of both end up getting into the nerves where they act to block pain. The difference in pH also means that mixing them likely slows the uptake of the lidocaine and might make the bupivacaine more likely to precipitate. Clinical studies in actual human and veterinary patients have also shown that this practice does not reduce the time to effect, but it does shorten the duration.
Steroids for Intervertebral Disk Disease (IVDD)
Acute medical management of IVDD mostly involves controlling pain and trying to prevent further injury or loss of function. Steroids have long been used for both analgesia and to protect from further deterioration of nerve tissue by reducing inflammation. Unfortunately, it has been difficult to produce research evidence that supports the real-world benefits of this approach. In humans, the use of oral steroids does not appear very beneficial, though it does have a higher incidence of adverse effects than other analgesics. The evidence in veterinary patient is sparse, but the most recent ACVIM consensus statement on the subject indicates that:28
- there is limited evidence that corticosteroid use is associated with poorer outcome and decreased quality of life as well as a higher rate of recurrence compared to nonsteroidal anti-inflammatory drugs (NSAIDs)
- [there is] insufficient evidence to support corticosteroid use for neuroprotective purposes
- In a retrospective study, dogs receiving NSAIDs had higher quality of life scores than those receiving corticosteroids
- there is not sufficient evidence to support the use of corticosteroids as a protective strategy against the development of progressive myelomalacia
The best we can say is that steroids are probably no better than NSAIDs, and it seems likely they may be worse.
MISCELLANEOUS TREATMENTS TO RECONSIDER
ACE Inhibitors for Pre-clinical Mitral Valve Disease
Diagnosis and staging of mitral valve disease (MMVD) before dogs are in congestive heart failure (CHF) is now pretty rewarding. The advent of pimobendane has given us an intervention that likely delays the onset of CHF and extend life significantly for dogs with this disease.29 It wasn’t always so.
Back in the Dark Ages that make up most of my career, we used to give these dogs ace inhibitors (ACE-I). There were some sound theoretical arguments to suggest this would slow the progression to CHF. Unfortunately, a few pesky scientists weren’t satisfied with theory, and they did some clinical studies in actual MMVD patients. They found that that we were most likely wasting our time.
As the most recent systematic review puts it, “Administration of angiotensin-converting enzyme inhibitors to dogs with preclinical myxomatous mitral valve disease…results in little to no difference in the risk of the development of congestive heart failure and may result in little to no difference in cardiovascular-related and all-cause mortality.”30
Good thing we’ve all stopped doing this, eh?
Glucosamine for Osteoarthritis (OA)
Probably the most popular (and profitable!) supplement in the history of veterinary medicine is glucosamine, alone or mixed with chondroitin or other agents. If everyone has used it forever, it has to work, right?!
Well, it turns out there is some controversy about that. Decades of research, hundreds of studies, are currently summarized in dozens of systematic reviews over the last ten years. For humans, these are often broken down into treatment for OA in specific joints, and there is sometimes analysis of glucosamine alone, in combination with other agents, or in different formulations and dosages. The result is muddled, and no clear, universal conclusions are possible.
About 60% of the reviews conclude there is some benefit to some type of glucosamine-containing product, and the other 40% conclude no meaningful benefit or insufficient evidence to tell. Not exactly a ringing endorsement for one of the most widely used supplements ever. The most recent systematic review for veterinary patients is ambivalent:31
“As we exposed in this review, glucosamine and chondroitin sulfate seems to provide chondroprotective effects and less inflammatory biochemical response in approximately half of the evaluations. However, these effects are inconsistent between the clinical and the preclinical studies… a possible caregiver placebo effect may explain some of the beneficial responses observed in clinical trials with dogs.”
The latest guideline from the American College of Rheumatology and the Arthritis Foundation, “recommends against glucosamine alone or with chondroitin because treatment does not improve knee and hip OA in studies without industry funding.”32 Ouch!
The American Academy of Orthopedic Surgeons say glucosamine “May be helpful in reducing pain and improving function…however, the research is inconsistent/limited.”33
There aren’t official guidelines from specialty groups in veterinary osteoarthritis management, but a recent proposed expert consensus statement highlighted the “lack of evidence” for efficacy needed to draw a firm conclusion.34 Another similar consensus statement indicated that three or four of nine contributing experts recommended offering some form of glucosamine for patients with OA depending on the specific circumstances.35
Despite being widely used for decades, it has proven impossible to clearly demonstrate that glucosamine in some form or combination has meaningful benefits for comfort and function in veterinary patients with OA. It is pretty well demonstrated to be safe, so there is unlikely to be any direct harm from using it. However, if it is ultimately not truly beneficial, what a horrendous waste of money it will have been for owners. And if it is used in place of clearly beneficial treatments (as it likely is, given how phobic people often are about NSAIDs), many OA patients could be suffering unnecessarily.
REFERENCES
1. Burton RA. On Being Certain: Believing You Are Right Even When You’re Not. 1st ed. St. Martin’s Press; 2008. Accessed April 3, 2024. http://catdir.loc.gov/catdir/enhancements/fy0829/2008001470-s.html
2. Gilovich T. How We Know What Isn’t so: The Fallibility of Human Reason in Everyday Life. 1. Free Press paperback ed. Free Press; 1993.
3. McKenzie B. Evidence-based veterinary medicine: What is it and why does it matter? Equine Vet Educ. 2014;26(9):451-452. doi:10.1111/eve.12216
4. McKenzie BA. Veterinary clinical decision-making: cognitive biases, external constraints, and strategies for improvement. J Am Vet Med Assoc. 2014;244(3):271-276. doi:10.2460/javma.244.3.271
5. Scahill K, Jessen LR, Prior C, et al. Efficacy of antimicrobial and nutraceutical treatment for canine acute diarrhoea: A systematic review and meta-analysis for European Network for Optimization of Antimicrobial Therapy (ENOVAT) guidelines. Vet J. 2024;303:106054. doi:10.1016/j.tvjl.2023.106054
6. Jensen AP, Bjørnvad CR. Clinical effect of probiotics in prevention or treatment of gastrointestinal disease in dogs: A systematic review. J Vet Intern Med. 2019;33(5):1849-1864. doi:10.1111/jvim.15554
7. Lappin MR, Zug A, Hovenga C, Gagne J, Cross E. Efficacy of feeding a diet containing a high concentration of mixed fiber sources for management of acute large bowel diarrhea in dogs in shelters. J Vet Intern Med. 2022;36(2):488-492. doi:10.1111/jvim.16360
8. Moreno AA, Parker VJ, Winston JA, Rudinsky AJ. Dietary fiber aids in the management of canine and feline gastrointestinal disease. J Am Vet Med Assoc. 2022;260(S3):S33-S45. doi:10.2460/javma.22.08.0351
9. Lappin MR, Blondeau J, Boothe D, et al. Antimicrobial use Guidelines for Treatment of Respiratory Tract Disease in Dogs and Cats: Antimicrobial Guidelines Working Group of the International Society for Companion Animal Infectious Diseases. J Vet Intern Med. 2017;31(2):279-294. doi:10.1111/jvim.14627
10. Bollig ER, Granick JL, Webb TL, Ward C, Beaudoin AL. A quarterly survey of antibiotic prescribing in small animal and equine practices—Minnesota and North Dakota, 2020. Zoonoses Public Health. 2022;69(7):864-874. doi:10.1111/zph.12979
11. Robbins SN, Goggs R, Lhermie G, Lalonde-Paul DF, Menard J. Antimicrobial Prescribing Practices in Small Animal Emergency and Critical Care. Front Vet Sci. 2020;7. doi:10.3389/fvets.2020.00110
12. Farrell S, Bagcigil AF, Chaintoutis SC, et al. A multinational survey of companion animal veterinary clinicians: How can antimicrobial stewardship guidelines be optimised for the target stakeholder? Vet J. 2024;303:106045. doi:10.1016/j.tvjl.2023.106045
13. Weese JS, Blondeau J, Boothe D, et al. International Society for Companion Animal Infectious Diseases (ISCAID) guidelines for the diagnosis and management of bacterial urinary tract infections in dogs and cats. Vet J. 2019;247:8-25. doi:10.1016/j.tvjl.2019.02.008
14. Dorsch R, Teichmann-Knorrn S, Sjetne Lund H. Urinary tract infection and subclinical bacteriuria in cats: A clinical update. J Feline Med Surg. 2019;21(11):1023-1038. doi:10.1177/1098612X19880435
15. He C, Fan K, Hao Z, Tang N, Li G, Wang S. Prevalence, Risk Factors, Pathophysiology, Potential Biomarkers and Management of Feline Idiopathic Cystitis: An Update Review. Front Vet Sci. 2022;9:900847. doi:10.3389/fvets.2022.900847
16. Williams J. Antimicrobial prophylaxis: The why and how of antimicrobial prophylaxis. BSAVA Companion. 2018;2018(11):4-7. doi:10.22233/20412495.1118.4
17. Davis E. The Use of Antibiotics in Veterinary Dentistry. Today’s Veterinary Practice. Published April 14, 2023. Accessed April 3, 2024. https://todaysveterinarypractice.com/dentistry/antibiotics-in-veterinary-dentistry/
18. Weese JS, Battersby I, Morrison J, Spofford N, Soltero-Rivera M. Antimicrobial use practices in canine and feline dental procedures performed in primary care veterinary practices in the United States. PLOS ONE. 2023;18(12):e0295070. doi:10.1371/journal.pone.0295070
19. Subedi M, Bajaj S, Kumar MS, Yc M. An overview of tramadol and its usage in pain management and future perspective. Biomed Pharmacother Biomedecine Pharmacother. 2019;111:443-451. doi:10.1016/j.biopha.2018.12.085
20. Benitez ME, Roush JK, KuKanich B, McMurphy R. Pharmacokinetics of hydrocodone and tramadol administered for control of postoperative pain in dogs following tibial plateau leveling osteotomy. Am J Vet Res. 2015;76(9):763-770. doi:10.2460/ajvr.76.9.763
21. Schütter AF, Tünsmeyer J, Kästner SBR. Influence of tramadol on acute thermal and mechanical cutaneous nociception in dogs. Vet Anaesth Analg. 2017;44(2):309-316. doi:10.1016/j.vaa.2016.02.003
22. Monteiro-Steagall BP, Steagall PVM, Lascelles BDX. Systematic review of nonsteroidal anti-inflammatory drug-induced adverse effects in dogs. J Vet Intern Med. 2013;27(5):1011-1019. doi:10.1111/jvim.12127
23. Donati PA, Tarragona L, Franco JVA, et al. Efficacy of tramadol for postoperative pain management in dogs: systematic review and meta-analysis. Vet Anaesth Analg. 2021;48(3):283-296. doi:10.1016/j.vaa.2021.01.003
24. Guedes AGP, Meadows JM, Pypendop BH, Johnson EG. Evaluation of tramadol for treatment of osteoarthritis in geriatric cats. J Am Vet Med Assoc. 2018;252(5):565-571. doi:10.2460/javma.252.5.565
25. Gruen ME, Lascelles BDX, Colleran E, et al. 2022 AAHA Pain Management Guidelines for Dogs and Cats. J Am Anim Hosp Assoc. 2022;58(2):55-76. doi:10.5326/JAAHA-MS-7292
26. Chincholkar M. Gabapentinoids: pharmacokinetics, pharmacodynamics and considerations for clinical practice. Br J Pain. 2020;14(2):104-114. doi:10.1177/2049463720912496
27. Hoffmeister E. Mixing local anesthetics – yay or nay? North American Veterinary Anesthesia Society. Published September 27, 2019. Accessed April 3, 2024. https://www.mynavas.org/post/mixing-local-anesthetics-yay-or-nay
28. Olby NJ, Moore SA, Brisson B, et al. ACVIM consensus statement on diagnosis and management of acute canine thoracolumbar intervertebral disc extrusion. J Vet Intern Med. 2022;36(5):1570-1596. doi:10.1111/jvim.16480
29. Boswood A, Häggström J, Gordon SG, et al. Effect of Pimobendan in Dogs with Preclinical Myxomatous Mitral Valve Disease and Cardiomegaly: The EPIC Study-A Randomized Clinical Trial. J Vet Intern Med. 2016;30(6):1765-1779. doi:10.1111/jvim.14586
30. Angiotensin?converting enzyme inhibitors in preclinical myxomatous mitral valve disease in dogs: systematic review and meta?analysis – Donati – 2022 – Journal of Small Animal Practice – Wiley Online Library. Accessed April 3, 2024. https://onlinelibrary.wiley.com/doi/10.1111/jsap.13461
31. Barbeau-Grégoire M, Otis C, Cournoyer A, Moreau M, Lussier B, Troncy E. A 2022 Systematic Review and Meta-Analysis of Enriched Therapeutic Diets and Nutraceuticals in Canine and Feline Osteoarthritis. Int J Mol Sci. 2022;23(18):10384. doi:10.3390/ijms231810384
32. Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020;72(2):149-162. doi:10.1002/acr.24131
33. Brophy RH, Fillingham YA. AAOS Clinical Practice Guideline Summary: Management of Osteoarthritis of the Knee (Nonarthroplasty), Third Edition. JAAOS – J Am Acad Orthop Surg. 2022;30(9):e721. doi:10.5435/JAAOS-D-21-01233
34. Mosley C, Edwards T, Romano L, et al. Proposed Canadian Consensus Guidelines on Osteoarthritis Treatment Based on OA-COAST Stages 1–4. Front Vet Sci. 2022;9. doi:10.3389/fvets.2022.830098
35. Cachon T, Frykman O, Innes JF, et al. COAST Development Group’s international consensus guidelines for the treatment of canine osteoarthritis. Front Vet Sci. 2023;10:1137888. doi:10.3389/fvets.2023.1137888