
Here are some low-quality recordings of a couple lectures I gave this year at the Western Veterinary Conference in Las Vegas.
A Book from the SkeptVet
Please follow & like us :)


 0
0








Here are some low-quality recordings of a couple lectures I gave this year at the Western Veterinary Conference in Las Vegas.
Back in 2011, I first wrote about the issue of concerning whether dogs with cranial cruciate ligament (CCL) ruptures did better with surgery or with non-surgical management. My conclusion at that time was:
For most dogs under 15kg, conservative management (primarily restricted activity for 3-6 weeks, achieving and maintaining and appropriate body weight, and possibly physical therapy and pain medication) can achieve acceptable comfort and function. In larger dogs, significant arthritis is inevitable and dysfunction is extremely likely without surgical treatment.
In 2013, I write an update looking at an additional study , and concluded:
This study does provide some support for the contention that overweight, large-breed or giant-breed dogs have better long-term outcomes when treated with both surgery and non-surgical therapy rather than with non-surgical therapy alone. However, the limitations in these data are great enough that the case for preferring surgical intervention is not strong
Since that time, there has been some further research, but there has not been one single, definitive clinical study comparing surgery with other approaches for managing CCL disease. This is partly for ethical reasons. Since most vets believe surgery produces a better outcome, it is considered unethical to randomly assign dogs with CCL disease to getting surgery or getting a potentially inferior treatment.
A new study has attempted to use existing data on a large number of dogs, and some complex analytic techniques, to mimic such a study.
Camilla Pegram, Karla Diaz-Ordaz, Dave C. Brodbelt, Yu-Mei Chang, Anna Frykfors von Hekkel, Chieh-Hsi Wu, David B. Church, Dan G. O’Neill. Target Trial Emulation: Does surgical versus non-surgical management of cranial cruciate ligament rupture in dogs cause different outcomes? Preventive Veterinary Medicine. 2024; 226;106165.
I don’t have the expertise to evaluate the analytic approach in this study. The authors acknowledge many of the usual limitations to large retrospective analyses, but despite these issues, such studies are valuable, especially I the evidence-poor environment of veterinary medicine.
The results are pretty consistent in showing better outcomes in dogs treated surgically:
The current study shows that on average, surgical management leads to reduced lameness and analgesic prescription outcomes compared with non-surgical management.

Interestingly, the study did not find any difference between large and small dogs. Both groups seemed to do better with surgery, which is a different finding than some previous research. The authors suggest this may be related to limited numbers of small dogs being treated, since they are less likely to develop CCL disease, so further work is needed to clarify the impact of size on the choice of treatment.
While there are always individual factors to integrate into any decision about the best management for a specific patient, this additional evidence tends to support the existing view that surgery probably produces better outcomes for dogs with CCL disease. While this is not the perfect definitive clinical trial, such a study is unlikely to occur. The evidence that we do have is pretty consistent, and it supports at least a moderate degree of confidence in recommending surgery for those patients in whom it is an option and who have no specific reasons to avoid surgical treatment.
One of the goals of this blog has always been to warn pet owners about dangers to their animals: dangerously unreliable ideas and ways of thinking about science and medicine, dangerous therapies (or at least those not yet proven to be safe or effective), and dangerous individuals who promote both unscientific approaches and unproven or unsafe treatments. There is remarkably little effective regulation and oversight of pet healthcare products, apart from prescription medications. Unscrupulous sellers of snake oil, including vets, can often get away with egregiously illegal and dangerous claims and practices.
Despite this, a few of the individuals I have warned pet owners about over the years have faced at least some legal or regulatory sanctions, though the process has been slow and has often not impeded their ability to sell their nonsense. Recently, one particularly bizarre example, Jonathan Nyce, has finally been sentenced to prison for selling fake cancer treatments for dogs, a decade after I started warning people about him.
This belated but positive outcome seemed like a good prompt for me to revisit some of the folks I have been writing about for some time who have faced official sanction for their abuse of science and the public’s trust. While the outcome in Mr. Nyce’s case is positive, the balance of these cases have not resulted in effective protection of the public and our pets.
Jonathan Nyce
My first post about Mr. Nyce was in 2014. In it, I looked at his claims for his supposed miracle cancer cure Tumexal (later renamed Naturasone). The product and the marketing had many of the hallmarks of quackery, from secret ingredients to use of testimonials and unpublished, potentially fabricated, test results. Mr. Nyce had a worrisome background, including previously questionable and unsuccessful attempts to market a drug for humans and a criminal conviction for murder, though I made a point of not making my critique of the product or the claims for it a personal critique of Mr. Nyce, since that is not a reliable way to judge such claims.
In 2020, I briefly reported on the criminal charges filed against Mr. Nyce for his illegal marketing of a fake cancer treatment. Finally, last month, Mr. Nyce was sentenced to 97 months in prison for his activities, which included bilking over 900 dog owners of nearly $1,000,000. Who knows how much harm his deception of well-meaning owners did to the patients themselves? As tempting as it is to rejoice at a well-deserved sentence, the more important question is whether this conviction will do anything to stop others from marketing bogus treatments. I have to admit to not being very optimistic on this point, for reasons which may be clearer as I review some other examples.
Gloria Dodd
Even before covering Jonathan Nyce’s misdeeds, I wrote about veterinarian Gloria Dodd in 2011 (not to be confused with Jean Dodds, about whom more later….). Dr. Dodd was a proponent of a broad array of pseudoscientific nonsense, from auras and homeopathy to crystal healing and dowsing. She was also a seller of many alternative remedies that were either entirely useless (e.g. homeopathic) or untested and based on unscientific principles.
Her practices were determined to cross legal lines more than once. In 2004, the FDA sent her a warning letter for selling a fake “homeopathic vaccine” for West Nile virus. That product was still available when I wrote about her in 2011.
She was also disciplined by the California Veterinary Medical Board for practices that were blatantly unscientific, “a smoke and mirror power of magic type of practice,” in the words of the VMB. Her license was suspended for prescribing treatments for patients she had never seen in person. However, the courts effectively overturned this ruling, and Dr. Dodds continued to practice her “magic” for years to come.
Dr. Dodd passed away in 2013, but her company continued to promote her ideas and products for several more years. Regardless of how kind and genuine a person Dr. Dodd may have been, it is tragic that she was able to mislead pet owners about health and veterinary medicine for decades and sell products that could not have been beneficial and may well have harmed patients, either directly or by replacing other, truly effective remedies. The failure of the legal and regulatory system to protect the public from such practices is disappointing, though not unusual.
Al Plechner
Dr. Plechner was another California veterinarian with deeply unscientific ideas about science and medicine. For decades, he treated patients for the mythical entity of “Plechner Syndrome” with high doses of steroids, thyroid hormones, Montmorillonite clay, and a variety of other nonsensical nostrums. While he claimed to have “research” to back his theories, he never published anything, and his descriptions sounded like nothing more than anecdotal case reports. Certainly, he never produced any evidence that convinced actual exerts in veterinary endocrinology that Plechner syndrome existed or had the causes and treatments he championed.
Like most purveyors of pseudoscience, Dr. Plechner did have dedicated supporters, who came out enthusiastically to “correct” me after my first post discussing his methods. His detractors, sadly, were less willing to go public. The private veterinary discussion boards on the Veterinary Information Network (VIN) contain many complaints and laments about Dr. Plechner’s ridiculous ideas, and about patients inappropriately treated with unsafe methods, but these never reached the public.
In 2015, I was contacted by an individual whose cat had been treated by Dr. Plechner with blatantly inappropriate doses of steroids. The cate suffered skin fragility syndrome (similar to this case) and faced surgery and a prolonged recovery from the effects of the drugs. Though several vets saw this cat and explained that the drugs were the cause of the problem, the owner had difficulty getting someone to support her complaint against Dr. Plechner, due to a combination of personal relationships between him and some of the vets and the general reluctance of veterinarians to call out even grossly inappropriate behavior by their colleagues.
The owner was able to find an internal medicine specialist to support her complaint to the VMB. Unfortunately, the wheels of justice ground slowly and started turning too late. Dr. Plechner retired and gave up his license in 2016. This did not automatically stop the VMB investigation, but Dr. Plechner then passed away in 2017, and no findings were ever released. However, his website is still active, his books are still for sale, and other vets (themselves with legal troubles) continue to promote his approach.
Jean Dodds
Dr. Dodds pops up often on this blog as she is a prominent voice in the alternative veterinary medicine arena, with lots of dubious ideas and unproven products and practices. I first mentioned her in 2011, in connection with some research on an oral health supplement, and I have provided detailed coverage of her unconvincing work on reduced “doses” of vaccinesfor small dogs (updated here), her unscientific and misleading writing about nutrigenomics, her bogus “allergy test” as well as other dubious tests she promotes, and many other topics.
Most recently, in 2021 I briefly discussed the citation against Dr. Dodds from the California Veterinary Medical Boardfor practicing medicine without a license, as she has done for many years. The citations was “satisfied” in August, 2023, presumably meaning she paid the fine and promised not to practice medicine (though I have not been able to find any no public record of how this was resolved). Despite this, Dr. Dodds profile, and the activity of her company, Hemopet (which itself has been fighting with the state over tax obligations) continue to operate openly and freely. The fact that her medical practice has been illegal for years does not seem to have lessened her influence or her business activities in any meaningful way.
Andrew Jones
Dr. Jones did not initially get his own post, but he popped up in passing in another article I wrote in 2010 as an example of the mania for magical “secrets” that alternative medicine proponents often claim to have for treating health problems that science-based medicine can’t cure. Later that year, Dr. Jones chose to give up his veterinary license rather than stop defaming veterinarians who practice mainstream medicine as a way of promoting his own alternative approach. It turned out Dr. Jones’ followers were even more aggressively supportive of their angry saint than those of Dr. Plechner, and when he rallied them, they went on the attack against me in all sorts of corners of the Internet. Several years later, Dr. jones was still perturbed by my criticism, and his supporters continue to leave comments on the blog more than ten years after my first article about him.
Of course, the reason for that is that losing his medical license has done nothing to deter Dr. Jones from selling his bogus “secrets,” and all sorts of products, online. The snake oil business is still booming, and many of his customers see him as a martyr rather than someone who couldn’t keep his medical practice consistent with science and the law. He proudly promotes his book, “From the #1 bestselling author and former practicing veterinarian,Andrew Jones DVM.” Bizarre! And while some do continue to push back against his pseudoscientific claims, Dr. Jones has a thriving career selling nonsense and lies despite no longer being licensed to practice medicine.
Eric Weisman
I first wrote about Mr. Weisman in 2009, the first year of this blog. His ideas about health and nutrition were bizarre and laden with extremist conspiracy theories, and his claims about the diets and practices he recommended were unscientific nonsense. He ultimately lost his chiropractic license and was sanctioned for practicing veterinary medicine without a license long before I started examining his claims. In 2011 he faced criminal charges for practicing human and animal medicine without a license and for animal cruelty. He reached a plea deal and got a slap on the wrist in 2012 despite his ling history of illegal and dangerously delusional behavior.
In 2018, he signed a stipulation from the Minnesota State Dept. of Public Health admitting to unlicensed practice of alternative medicine and misrepresenting his credentials and promising not to do it again. He also paid a $263 fine. In the most bizarre legal resolution to any of these cases I have yet seen, doing this apparently allows Mr. Weisman to do whatever bizarre voodoo he likes with the permission of the Minnesota state government:
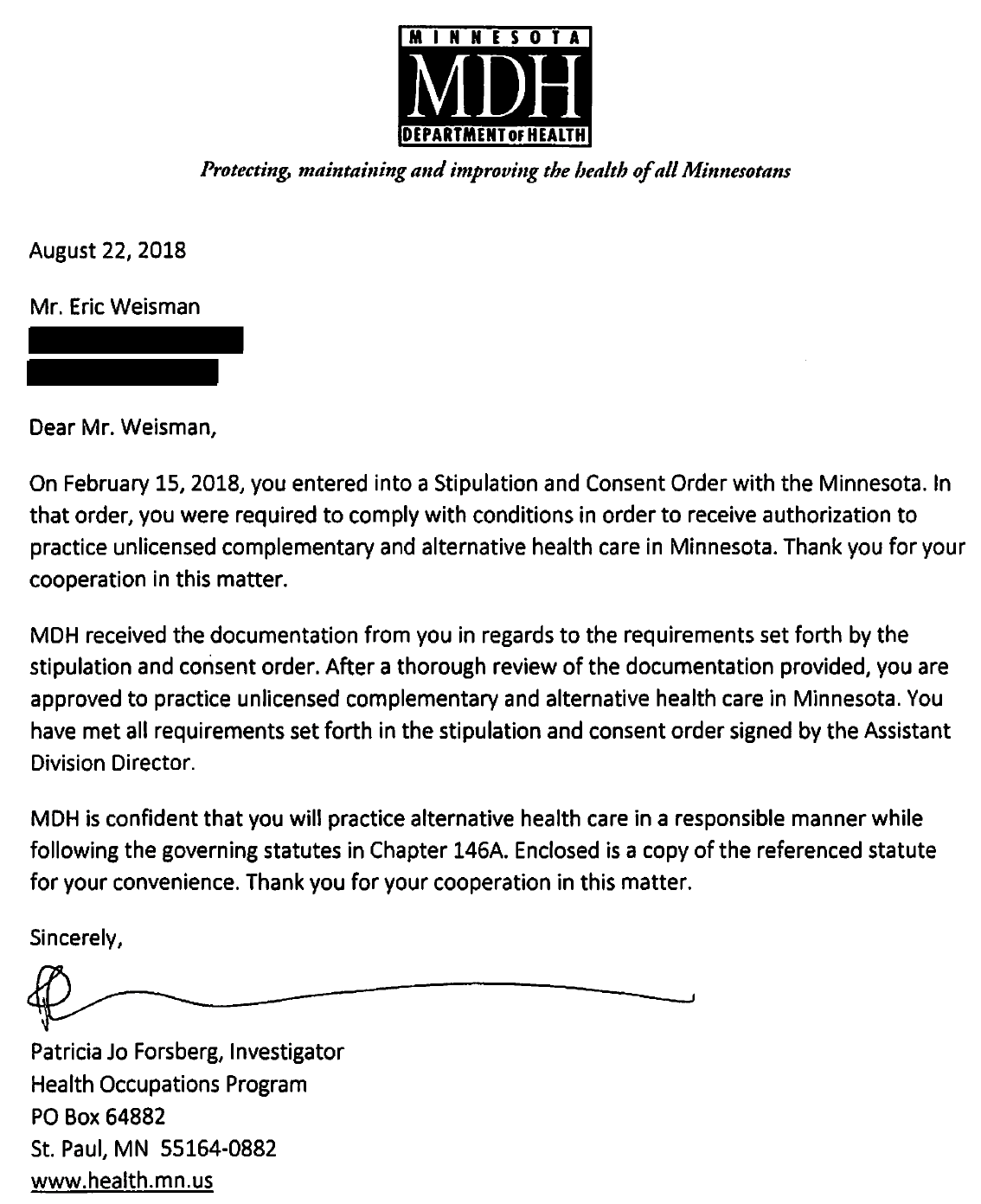
It turns out that the government of Minnesota has entirely given up any pretense of protecting the public from charlatans and witchcraft. Mr. Weisman is doing just as he pleases, offering “consultations:” as well as selling vegan pet food with longevity claims based on a grossly misleading and unscientific interpretation of some published owner survey reports.

Apparently, claiming to be able to treat serious life-threatening illnesses, interpret clinical lab tests and MRI images, and discouraging patients from seeing legitimate, science-based medical practitioners is now A-OK in Minnesota! Yet another quack thriving by deceiving the public.
Back in January of 2023 I reviewed claims for a purported anti-aging supplement for dogs called Leap Years. My conclusion at the time was-
Leap Years is similar to most veterinary supplements on the market: It is based on some plausible ideas with limited supporting evidence, and it is marketed with claims that go well beyond anything scientifically proven or reasonable.
In that review, I pointed out that one piece of evidence the manufacturer cited to support their claims was an unpublished clinical study conducted at the veterinary school at North Carolina State University (NCSU). That study is still has not been published in a peer-reviewed journal, but the company has recently released a report on the preprint service Bioarxiv.
This is an increasingly common practice which is supposedly intended to make important information available more quickly, but which in most cases has more public relations value than scientific value. Until a paper is put through peer-review, it has only been critically evaluated by the authors or people they have chosen, which leaves lots of opportunity for bias. Such preprints may change significantly before publication or even never be peer-reviewed and published at all.
Preprints are clearly a lower level of evidence than full published research reports, but they do at least provide more detail for anyone interested in evaluating the research and claims made using it. As you have probably already guessed, that’s what I intend to do here!
The Study
The study was a blinded, randomized, placebo-controlled clinical trial conducted in accordance with appropriate methodological guidelines, which is always nice to see. The authors do a good job of describing the methods, including the bias-control practices, progress of subjects through the trial, and the potential limitations. The one critical piece of information missing is the actual chemical compounds used in the supplement.
As discussed in my previous review, Leap Years supposedly contains an NAD+ booster, which the company states is not NMN but otherwise does not identify. This was given daily for the duration of the 6-month study period. The supplement is also claimed to contain a senolytic, which is also not identified and which was given on two consecutive days each month during the study.
The FDA is pretty clear that veterinary supplements are not covered under the limited regulatory rules for human supplements (the Dietary Supplement Health and Education Act or DSHEA). Anything marketed for animals must either be a food or a drug. Leap Years is clearly not a food, and the claims made for it very much sound like treatment claims for a veterinary drugs:
[Leap years] significantly improves owner-assessed cognitive function and may have broader effects on frailty, activity and happiness as reported by owners.
That would make it seem like the company is marketing an unlicensed veterinary drug without first demonstrating safety and efficacy, as is required. However, the FDA does not seem to have the resources or political backing to effectively enforce these rules, and the same is true for many other veterinary supplements. Legal or not, it seems to me unethical (if not unusual) to market a supplement with undisclosed ingredients and claim that it prevents or treats serious health problems in dogs. This study does nothing to address that concern.
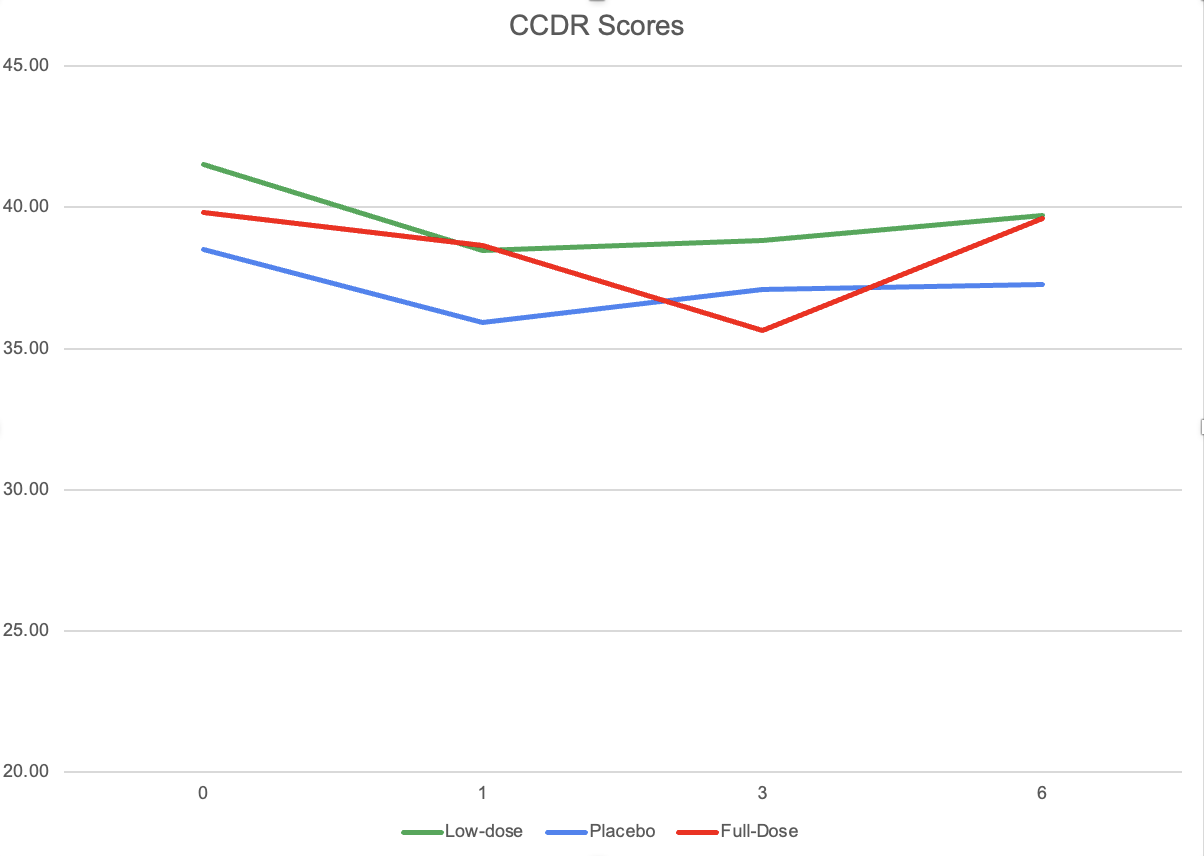
The trial started with 67 dogs randomized to placebo, low-dose supplement, and high-dose supplement (though the authors refer to these as “low-dose” and “full-dose,” which seems an obvious attempt to avoid the potential negative connotations and anxiety that might come with claiming to provide a “high” dose of whatever the undisclosed ingredients are). Subjects dropped out at various stages of the study for a variety of reasons. The total dropout rate was a bit high (19-26% from baseline to final analysis of the data), as is to be expected with an already old population. However, the dropouts seemed roughly balanced across groups, so while this might have affected the statistical power of the study, it probably didn’t bias the results for or against any of the treatments.
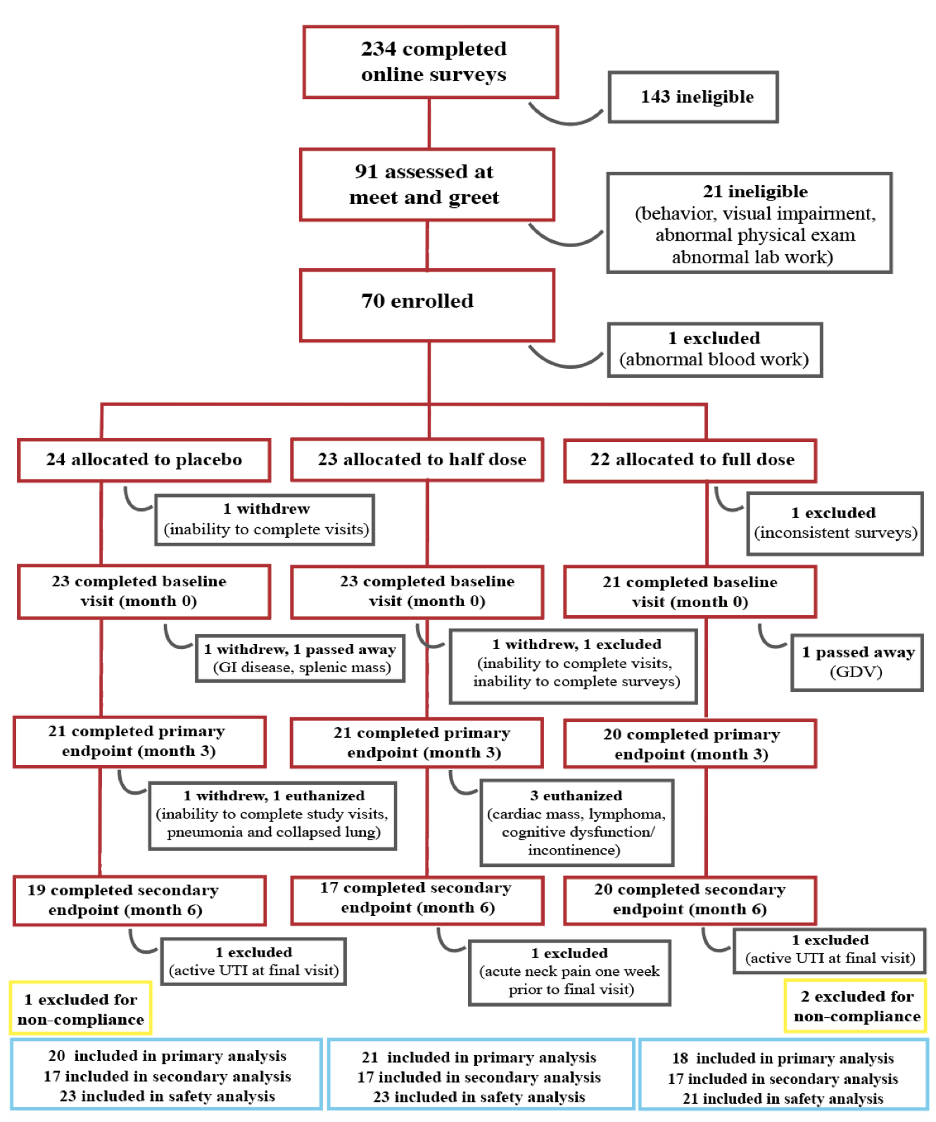
The dogs were included in the study if they were at least 10 years old and had mild or moderate cognitive dysfunction as assessed by a validated tool (CADES). They also had to be cooperative for behavioral testing and not so sick or debilitated that they couldn’t complete the various evaluations of the length of the study. All of these are reasonable inclusion criteria.
There were quite a few outcomes measured, though at least these were appropriately identified as a primary outcome (which is all that is supposed to matter when one critically evaluates a study like this) and secondary outcomes (which are supposed to be viewed as potentially interesting but not probative).
The primary outcome was the change at 3 months in a validated measure of canine cognitive dysfunction (CCDR, not the same as used to test dogs for inclusion in the study). As the figure below shows, all groups improved, including those taking a placebo, which is a classic finding for non-specific effects of participating in a clinical study. Patients tend to get better due, most likely, to the increased care, attention, and monitoring they get as study subjects, even if the treatment doesn’t do anything (which is part of why having a placebo group is so important).
At 3 months, the placebo group looks better than the low-dose group, and the high-dose group looks better than both, and the authors report, “There was a significant difference between treatment groups over the three-month period (p=0.02).” However, differences in “successes” and “failures” (improvement or worsening of CCDR scores) between groups were not significant at 3 months.
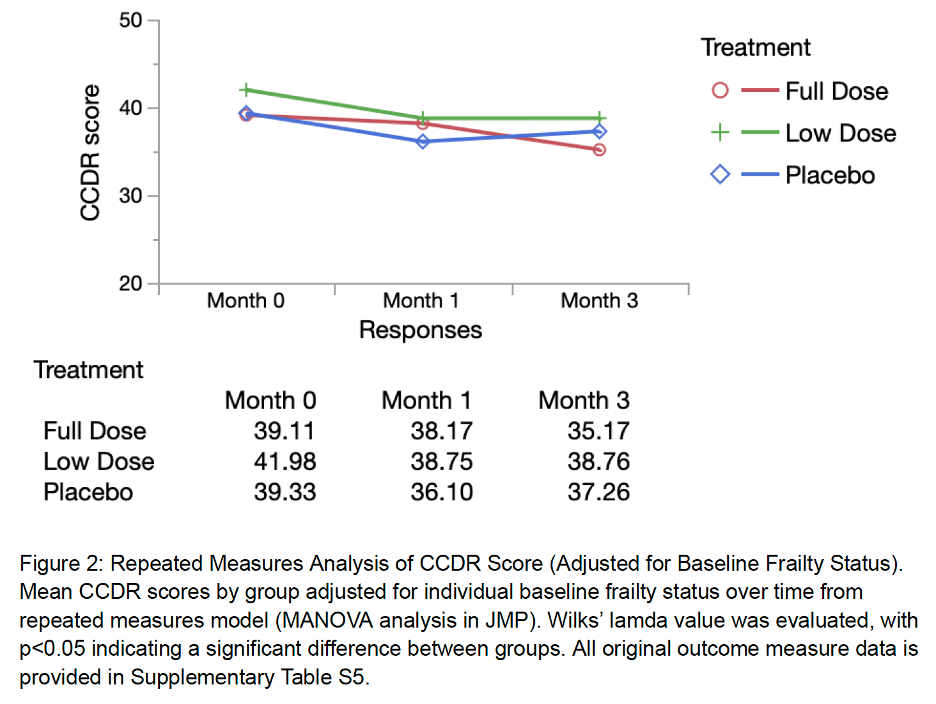
More importantly, it’s not clear if these differences would be meaningful in terms of function or quality of life even if they were statistically significant. It is not even clear that these differences are real since they are variable across time periods and do not show the expected relationship between dose and response (the placebo group should stay the same or get worse, the low-dose group should get a little better, and the full-dose group should improve more than the low-dose group).
Expanding the chart to include the data from the 6-month timepoints (reported in the supplement to the preprint) shows the lack of these relationships and suggests that there is not clear and meaningful improvement with the supplement. Even though the 3-month timepoints was reported as a prespecified endpoint, it is interesting that it is the only timepoints that seems to show a significant improvement in a treated group and not the placebo group. Despite the statistical difference reported, it is pretty clear that the primary endpoint did not show the treatment to be effective.
The secondary outcomes also failed to show any clear evidence of a beneficial effect:
The authors also monitored for adverse effects and classified these according to appropriate standards. There were few serious adverse effects observed, and these were evenly distributed between the groups and did not suggest any dramatic safety problems with the product.
Bottom Line
This report does not count as a peer-reviewed publication, and it adds only a little to the evidence already discussed a year ago to support the product claims. However, the report is useful in that it provides more detail about how the study was conducted and what the results were. Generally, the study was designed and reported appropriately, and the level of control, for bias was pretty good. Unfortunately for the company, the results failed to show statistically significant or clearly meaningful benefits for treated dogs.
The discussion and the company website, of course, try to present the findings in at least a slightly positive light, but the final statement that the product, “can be used safely to mitigate cognitive decline in senior dogs and might have broader effects on dog health manifesting as improved happiness and reduced frailty” is certainly not supported by the actual results reported here. The best we can say is that there were no apparent signs of significant risk and there were a few non-significant findings that might turn out to be mildly beneficial at a low but significant level in a larger study or with different outcome measures.
This level of evidence is never the definitive word for or against a treatment, but that this is the best the company can come up with after over a year on the market is not encouraging. The company makes claims which seem likely to be prohibited for a veterinary supplement, and they rely on anecdote and questionable extrapolation from theoretical science and results in other species to market the product, and the release of this study does nothing to strengthen their case.
March 12, 2024- Addendum
Today Dr. Nir Barzilai announced that Dr. Sinclair was resigning from the presidency of the Academy for Health and Lifespan Research. It is nice to see some consequences for such clear, commercially motivated misuse of science. Hopefully, this will encourage Dr. Sinclair to focus more on research and less on selling unproven supplements, for dogs or humans!

As I’ve mentioned previously, in the last four years I have continued my clinical practice while also working for Loyal, a biotechnology company pursuing FDA approval of drugs to extend health lifespan in dogs. There is little overlap between my SkeptVet activities and my work at Loyal, and of course my writing here doesn’t represent the official position of the company on anything. But I do like to share here some of the science and publications on aging that I work on at the company. Sadly, that tends to draw the attention of those irritated by my advocacy for science-based veterinary medicine.
Recently, there was a large amount of publicity surrounding a milestone on the road to potentially getting our first drug approved at Loyal. While this drew mostly positive interest, I was accosted on the SkeptVet Facebook page by a follower of the “holistic veterinarian” Dr. Judy Morgan. Dr. Morgan’s fan asked me to respond to a FB Live video briefly discussing (or “ranting about,” in Dr. Morgan’s own characterization) the press coverage of Loyal’s work.
I eventually had to block this fan’s account for personal abuse, and I don’t generally bother to respond to trolls since their comments are typically ignorant and disingenuous, and their minds are firmly closed. Dr. Morgan’s fan wanted to set up a “debate” between us, a common tactic among alternative medicine advocates that mistakes theatrical performance for substantive exploration of evidence-based science. As I explained to her on FB, “science isn’t about public debate or performance, its about evidence. [Dr. Morgan] can say what she likes, and support it with whatever evidence she has, and I can do the same, and everyone can evaluate her claims and support for themselves…How we sound or look on video talking to each other isn’t useful or relevant, it’s just theater.”
However, there are some pretty significant misconceptions and misrepresentations of science and the drug approval process generally in Dr. Morgan’s video, and I thought it might be useful to take the opportunity to respond to those and, hopefully, give everyone a clearer picture of how those processes work and how science gives us the best chance at finding therapies that provide meaningful, beneficial impact on the health and wellbeing of our pets.
What Was the Fuss About?
The announcement and associated publicity concerned something called Reasonable Expectation of Efficacy (RXE). This is a standard for supporting evidence that the FDA sets for veterinary drugs as part of the process of pursuing conditional approval. Since the regulatory system is complex and not something vets or pet owners often know much about (I certainly didn’t before becoming involved in this project!), I thought I’d start with a brief outline of how it works. The official explanation and detains can be found on the FDA web site.
Any medicine intended to treat disease in animals must be approved by the FDA. This is to ensure that these medicines are both safe and effective. Of course, as I’ve said many, many times, nothing is ever perfectly safe or always effective, and medicine is about balancing the benefits of a treatment against the potential risks, all in the light of the available scientific evidence and the frustrating, but inevitable, uncertainty about these. Having FDA approval means that a significant degree of scientific evidence at multiple levels is available to support the specific claims of safety and efficacy made for a prescription drug. This is not perfect, but it’s a great deal better than what is available for treatments that don’t go through this process (including supplements and nearly all forms of “alternative” medical treatments).
In the case of the typical FDA approval process, the agency requires several types of supporting evidence for safety and effectiveness. This includes pre-clinical research, that is studies done in test tubes or lab animals showing how a drug works and what biological effects it has. Such studies are an important part of demonstrating what we call “biologic plausibility,” the existence of an explanation for how something works that is consistent with established scientific knowledge.
Therapies such as homeopathy or “energy medicine” (such as Reiki) lack biologic plausibility because there is no scientific rationale for how they might work; they can only work if much of what we know about basic physical, chemistry, and biology is wrong. While scientific knowledge isn’t always completely correct, the basic knowledge that is the foundation for most of the successful medicine and technology in use today is pretty unlikely to be completely wrong. Clinical studies of these implausible therapies don’t make much sense and are often misleading.
Once there is good evidence for the underlying biology of how a drug might work, then a company seeking approval has to test it directly in the species it is intended for. If the drug is being developed for dogs, then studies must be done in dogs to understand how the drug works and what risks it may have. Sometimes this involves studies in laboratory dogs, often beagles, but it may also involve research in companion dogs. These studies have to comply with rigorous guidelines for methodology and to control various types of bias and error, so they are usually stronger evidence than studies not performed under such guidelines.
Finally, if the evidence to this point shows the drug is likely to be safe and effective for its intended purpose, a clinical trial is performed. This is the “randomized controlled trial” or RCT that people most often associate with medical science, even though it is only one part of a much more comprehensive testing process. In an RCT, ideally some dogs are given the new drug and others are given a placebo (a “fake” drug which does nothing at all), and everyone involved is “blinded” so they don’t know which is which. The details vary with the specific drug being tested, but again the standards for how these RCTs must be conducted to gain FDA approval are very specific and quite high, so the results are pretty good quality evidence.
This process often takes many years and is very expensive to complete. This is a problem because it makes it harder for veterinarians to get new and properly tested therapies. The system in most countries, and certainly in the U.S., is set up so that private companies are responsible for paying the costs of developing and testing new drugs, and so they aren’t likely to do so unless they think they can make back the money invested in this. Lots of interesting political debates could be had over whether a different system would be better, but that’s beyond the scope of this blog, and frankly nothing about this is likely to change here any time soon.
The FDA recognizes that vets can’t get many treatments that have met the high standards of the typical approval process, and so it allows some compromises to make useful therapies available to vets and their patients. We are, for example, allowed to use drugs approved for humans “off-label,” meaning in ways they were not tested and approved for. Many of the treatments vets use have been tested thoroughly for safety and efficacy in humans but not in dogs or cats. While this increases the potential risks when we use them in these species, often this is still better than the alternative of having no treatment for a given problem, or having treatments that haven’t even been scientifically validated in any species.
The FDA also doesn’t regulate some treatments much at all. The rules governing dietary supplements are especially lax (and violated all the time with little consequence), so it is much faster and more profitable for companies to make supplements than develop prescription drugs. Sadly, this has led to a booming and lucrative industry (highly favored by alternative medicine advocates like Dr. Morgan) selling products that may be claimed to be safe or effective even when there is little to no real evidence that these claims are true.
A more recent change in the FDA approval system has been the pathway of conditional approval. Under this approach, new drugs must meet all the same requirements for proving safety, manufacturing quality, environmental impacts, and so on as under full approval. However, if a product is targeting a serious health problem with no existing effective treatments (which is clearly the case for aging), and if the RCT needed for full approval is complex and likely to take a long time (again, this is clearly true for drugs intended to extend healthy lifespan), then a drug can be made available to vets for use while that RCT is being conducted.
In order to do this, the company must provide sufficient evidence that the product is likely to be effective (aka reasonable expectation of efficacy or RXE) along with the usual evidence for safety and other components of approval. Several products have been made available to vets under this pathway, including medications for heart disease, pancreatitis,anemia, and epilepsy.
The big news in the press that prompted Dr. Morgan’s “rant” on FB was that the FDA granted this RXE approval for one of Loyal’s products. The support for this approval included four years of pre-clinical research and 2,300 pages of data and documentation, so it is a pretty robust standard even prior to the completion of the final RCT. The product has not yet been approved, and it is not expected to be available for at least another year even if it eventually achieves this approval. However, the milestone was pretty significant since the FDA has never before granted RXE status (or approval of any kind) for a drug intended to treat the mechanisms and consequences of aging. Ultimately, this has the potential to open up an entire new area of preventative medicine, though there is a long way yet to go towards this goal.
Who is Judy Morgan?
Dr. Morgan is a self-described “holistic” veterinarian. She was in clinical practice for many years, and since retiring she has focused exclusively on selling products, books, and educational courses on her web site as well as a variety of other educational and advocacy activities. She is quite typical of the alternative medicine advocates I have written about many times. She promotes Traditional Chinese Veterinary Medicine (TCVM), homeopathy, raw diets, innumerable untested supplements, and a wide range of dubious or disproven tests and treatments. She is also deeply suspicious of science-based veterinary medicine, condemning conventional diets and ranting about the dangers of conventional drugs, vaccines, parasite preventatives, and other mainstream medical tools.
Her educational courses often touch on longevity and geriatrics, and she clearly has an interest in these areas. However, her advice is largely unscientific, and she makes numerous false claims about the “proven” benefits of raw diets, TCVM, supplements, and so on. Anyone who suggests vets should choose supplements and foods for maintaining health or treating disease based on supporting “elements” such as Fire, Wood, and Water, or on “balancing” mystical energies like Yin and Yang, cannot be taken very seriously when commenting on science and scientific medicine.
What’s the “Rant” About?
Most of Dr. Morgan’s video has nothing to do with Loyal’s products or the related media coverage. She spends much of her time talking about the work of a Japanese scientist on apoptosis inhibitor of macrophages (AIM), a protein supposedly being developed into a dietary supplement or injectable medicine to prevent or treat kidney disease and extend lifespan in cats (a set of claims that are themselves pretty dubious, and which I will try to find the time to talk about someday).
Unfortunately, she doesn’t make the transition very clear when she switches from talking about the Loyal RXE coverage and other subjects, and she repeatedly talks about a “vaccine” for aging, although neither Loyal nor the Japanese scientist she discusses are developing a vaccine. This may just be a sloppy shorthand for anything injectable, or a superficial reading of the media coverage (one web site does describe the AIM product as a “vaccine,” though the actual company web site makes it clear that is not what is being developed.) However, since she does spend a fair bit of her time talking about the dangers of vaccines (while still claiming to support them), I think this is part of the obvious effort she is making with this video to cast these products in a suspicious light for her viewers, many of whom are likely as distrustful of vaccines as she is.
Dr. Morgan begins the video by suggesting that she isn’t impressed by the RXE approval and she is “gonna wait ten years and see what the reports are” before even considering using this or any other drug treatment for aging. This is part of a consistent theme throughout the video– suspicion of scientific evidence and a preference for anecdotes to evaluate medical treatments. At one point, she actually says, “one of the great ways to find out what side-effects can be seen is social media.” ???? In her view, “if people are reporting the same side-effect time after time after time” then this is a reliable indicator of the safety of a drug. This ignores the well-established unreliability of anecdotal evidence (as the saying goes, the plural of ‘anecdote’ is not ‘data’).
She clearly doesn’t understand the role of pre-clinical evidence, not only because she recommends therapies that fail to show basic biologic plausibility, but because she acts as if any use of a drug without a comprehensive RCT is a dangerous experiment. With regard to conditionally approved drugs, she says, “When you go to your vet the day this thing hits the market, your dog is part of that clinical trial, you are saying, Yes, I am going to let my dog be part of that science experiment…it might have some serious side-effects that we don’t know about.”
One could claim that she is simply demanding the highest form of evidence for medical treatments, except that clearly she is comfortable using supplements, diets, and alternative therapies that have never been shown to be safe or effective through clinical trials. What is more, she explicitly admits she would never participate in a clinical trial because she thinks they are too dangerous: “I will not sign my dogs up for clinical trials. I know somebody has to somewhere but it’s not gonna be me.” Instead, she has the bizarre but common belief that scientific evidence is unreliable but if we have enough anecdotes then we can know what therapies are safe or effective. That is the sort of fundamental misunderstanding underlies so much of alternative medicine, and it makes her judgements on specific interventions unreliable.
Consistent with this approach, she often makes false claims about the risks of lack of efficacy of treatments based on anecdotal reports collected online. For example, she claims that isoxzoline parasite preventatives “have killed hundreds of thousands of animals” based on such reports, which is a demonstrably untrue exaggeration (e.g. 1, 2, 3). She also argues that the allergy treatment lokivetmab (a.k.a. Cytopoint) commonly ceases to work because of anti-drug antibody formation (for which there is no substantive evidence) and that there are “tons of side-effects” but the company “[doesn’t] have to report the side-effects that are seen once the drug is used widely,” which is again completely untrue.
Bottom Line
None of the drugs Loyal is developing have been approved for use by the FDA, so of course no one is claiming they have been proven to be safe and effective yet. Having strong scientific evidence at all levels is the whole purpose of going through the prescription drug approval process rather than just launching a longevity supplement, which is a much faster and easier way to get a product to market with minimal scientific evidence. More evidence is needed, and it is being generated.
However, it is clear that better scientific evidence is not really what Dr. Morgan is concerned about. She already believes she can extend lifespan and healthspan with therapies that don’t have any meaningful scientific support, such as raw diets, supplements, and TCVM. And she repeatedly rejects the evidence when it is favorable to treatments she believes are dangerous base don anecdote or just simple prejudice against “injections” and “chemicals” and so on.
Hopefully, veterinarians and dog owners with a genuine interest in aging and in prolonging healthy lifespan will be interested in any new tools that are developed to achieve this. Hopefully they will critically evaluate the strengths and limitations of the scientific evidence as we all should for all of the therapies we use. However some, and I suspect Dr. Morgan will be one, will automatically reject any pharmaceutical as a safe and effective way of extending healthspan regardless of the evidence because it doesn’t fit their fundamentally unscientific philosophy. That’s fair enough, of course, but those folks shouldn’t try to claim that this rejection is really about holding out for more and better evidence if this is obviously inconsistent with their other claims and practices.
The American Veterinary Medical Association (AVMA) functions mostly as a lobby and PR organization for veterinarians. It is a membership organization and, as such, is beholden to whoever its members are, and the organization is very keen to avoid conflict within the profession or any suggestion of forcing vets to do anything in particular. The wild political drama surrounding a simple resolution in the AVMA House of Delegates to acknowledge the demonstrable uselessness of homeopathy demonstrates this quite starkly.
The AVMA does make some attempts to promote standards “within the family,” generally in the form of non-binding position statements. These are often pretty lukewarm compromises between competing interests, but they have some utility. The AVMA also has a Principles of Veterinary Medical Ethics, and the organization is currently asking for comments from members on a proposed Code of Conduct based on these principles.
This document does offer some acknowledgement of the importance of evidence-based medicine for ethical clinical practice, and it seems possible that this could be strengthened somewhat, though I am not extremely optimistic. Nevertheless, I encourage any readers who are AVMA members to participate in this comment period, and anyone else to consider encouraging any members you know to do so.
Here is the draft code of conduct.
The commenting period will close at 11:59 p.m. Central Time on March 4, 2024.
Here are the comments I made
Section B
subsection 1
paragraph d
“A veterinarian does not have an ethical obligation to deliver care requested by a client that they believe would cause unnecessary pain and suffering for the patient and that is unlikely to be beneficial.”
A veterinarian has an ethical obligation to prioritize offering evidence-based care that is most likely to be beneficial and that maximizes the ratio of likely benefit to potential harms.
Recommendation:
I recommend adding the language in bold to this section.
Rationale:
The purpose of a code of conduct is to articulate “specific types of behaviors that are either expected or required of members of the veterinary profession,” not merely those behaviors that are not expected. This section indirectly indicates that veterinarians should prioritize care that is likely to be beneficial or with likely benefits that outweigh potential harms, yet it does not clearly articulate a positive expectation for the corresponding behavior. The section should indicate that the ethical behavior is to prioritize and offer only care which is expected to have benefits greater than its risks.
Section B
subsection 2
Evidence?based Medicine
“A veterinarian should prioritize the delivery of evidence?based medicine and should inform the client when a therapy does not meet this standard.”
A veterinarian should eschew practices that do not meet a reasonable standard of evidence for safety and efficacy.
Recommendation:
I recommend adding the language in bold to this section.
Rationale:
The guidelines recognize that there is an ethical obligation to “prioritize evidence-based care” because this is the type of car most likely to benefit patients. If this is true, it is not sufficient to simply inform clients when we are offering care that does not meet this standard and then offer care that is not evidence-based or not likely to be safe and effective anyway. Veterinarians should be expected to eschew practices that are unlikely to have benefits greater than their risks based on a reasonable standard of evidence.
General practice veterinarians (GPs) are often faced with the question of which services they should provide themselves and which should be left to board-certified specialists. The growing availability of specialty care, the expectations of many pet owners for advanced care resembling that which they receive, the expanding availability of new and more technologically sophisticated interventions, and many other factors all add to the pressure to limit services in general practice and refer more patients to specialists.
On the other hand, many pet owners struggle to find and afford veterinary care of any kind, much less the most advanced. The concept of a spectrum of care has gained momentum in veterinary medicine largely in acknowledgment of this and in recognition of the fact that intensive, technologically sophisticated, and expensive healthcare may not always be available and may not even the best option for a given patient and client. I was privileged to be invited to contribute to one of the first attempts to characterize the concept of a spectrum of care in the veterinary literature, and it has gained significant momentum since (e.g. 1, 2)
One element to the spectrum-of-care concept is allowing flexibility in what care is provided and by whom while still providing effective, evidence-based treatment. General practice vets are very experienced at the art of providing care within the many constraints of time, money, and expertise available in private practice.
Unfortunately, sometimes both GPs and specialists, especially some in academic settings, mistake the most intensive and advanced specialty care for the best care, or even for the only acceptable kind of care. This makes it harder for GPs to meet the needs of their patients and clients within the inevitable limitations of the “real world,” that is, practice outside of universities or highly affluent communities.
I have been fortunate enough to work for many years at a practice where I was able to learn and provide advanced care options often considered the exclusive province of specialists, such as endoscopy, chemotherapy, and ultrasound. While some specialists have objected to this, many have understood the importance of avoiding rigid distinctions between primary and specialty care in order to effectively meet the needs of all our patients and clients.
Recently, I have developed the impression that newer veterinary school graduates are more reluctant that earlier generations to provide such advanced care tasks. Whether this is a generational change or a result of the messages they are receiving in school, such a trend could potentially further limit the availability of high-quality care and exacerbate both the shortage of veterinary services and the dissatisfaction driving vets from clinical practice.
I recently wrote an editorial for the Journal of the American Veterinary Medical Association (JAVMA) intended to explore the issue of specialty referral, and to hopefully advance discussions within the profession around this subject. This is based solely on my own experiences in practice, and my understanding of evidence-based medicine and the spectrum of care concept, so it is only my thoughts on the subject, not an objective, data-driven analysis. Nevertheless, I hope this will provide useful context and food for thought to GPs and specialists, and perhaps to pet owners as well.
McKenzie, BA. Do it yourself or send for help? Considering specialty referral from a general practitioner perspective. J Amer Vet Med Assoc. 2024; Online early. doi: 10.2460/javma.23.11.0612
It’s been ten years since my first post on the use of cannabis in dogs and cats. For a while, I regularly covered new research studies, but the number of those has become great enough that keeping up with individual papers is not feasible. Fortunately, the principles of evidence-based have an answer- literature reviews!
There are two main types of review articles of use to clinicians: narrative reviews and systematic reviews. Narrative reviews are far more common in veterinary medicine. These involve individuals or small groups reviewing the research on a given subject and writing a summary from their perspective. These reviews can be very useful, and I have written several myself. But of course they are subject to significant bias. Authors can choose which studies to include and which to ignore, and they can interpret the results through the lens of their existing beliefs on the subject. This doesn’t mean narrative reviews are not useful, but it is a reason for caution in the level of confidence we place in their conclusions.
Systematic reviews are more formal projects, with clear and explicit standards to encourage a comprehensive assessment of the research on a given subject and an objective summary of the strength of the evidence. These are less subject to bias, but they have the weaknesses of often being inconclusive. When there are few studies or most research has significant limitations, no confident conclusion is justified, and most systematic reviews end with the conclusion that more research is needed. This is especially the case in veterinary medicine, where having only a few small studies with significant methodological limitations is the rule.
In the case of veterinary cannabis, there are only a few systematic reviews. One has looked specifically at the literature for cannabidiol (CBD) use in dogs with osteoarthritis (OA).
Patikorn C, Nerapusee O, Soontornvipart K, Lawonyawut K, Musikpodok K, Waleethanaphan K, Anantachoti P. Efficacy and safety of cannabidiol for the treatment of canine osteoarthritis: a systematic review and meta-analysis of animal intervention studies. Front Vet Sci. 2023 Sep 15;10:1248417. doi: 10.3389/fvets.2023.1248417. PMID: 37781283; PMCID: PMC10540436.
As expected, this review had to rely on only a few studies (five), and “All studies were rated as having a high risk of bias.” The conclusion was that CBD “may reduce pain…but the certainty of evidence was very low.” Fortunately, “CBD is generally considered safe and well-tolerated in the short-run, with few mild adverse events observed, such as vomiting and asymptomatic increase in alkaline phosphatase level.” However, as usual the bottom line is that more and better research is needed to allow any confident conclusions about the utility of CBD in arthritis dogs.
A slightly older review looks at all uses of cannabis in dogs.
Lima TM, Santiago NR, Alves ECR, Chaves DSA, Visacri MB. Use of cannabis in the treatment of animals: a systematic review of randomized clinical trials. Anim Health Res Rev. 2022 Jun;23(1):25-38. doi: 10.1017/S1466252321000189. Epub 2022 Jun 15. PMID: 35703023.
Only six studies met the criteria for quality to be included, all in dogs “with osteoarthritis (n = 4), with epilepsy (n = 1), and with behavioral disorders (n = 1)” and all using CBD as the test treatment. All studies showed improvement in the conditions being treated, but “studies were heterogeneous and presented risks of bias that required caution in the interpretation of findings.” As in the more recent study, “CBD was well tolerated with mild adverse effects,” but “More RCTs with high quality of evidence are needed, including greater numbers of animal subjects, additional species, and clear readout measures to confirm these findings.”
A few narrative reviews have also appeared in the last couple of years that provide a good overview of the uses and evidence for cannabis-based remedies in veterinary medicine. The most comprehensive looks at dogs and cats.
Corsato Alvarenga I, Panickar KS, Hess H, McGrath S. Scientific Validation of Cannabidiol for Management of Dog and Cat Diseases. Annu Rev Anim Biosci. 2023 Feb 15;11:227-246. doi: 10.1146/annurev-animal-081122-070236. PMID: 36790884.
One interesting lesson from this review is that despite severely limited evidence and great uncertainty about what cannabis products might be useful for at what doses with what risks, people are using them all the time for everything. The perception appears to be that cannabis is a safe and effective panacea for companion animals, which of course isn’t substantiated by the actual evidence.
“The cannabidiol (CBD) pet market is expected to increase by $3.05 billion during 2021–2025, with a compound annual growth forecast to reach nearly 30%…A survey conducted online in the United States reported that nearly 60% of pet owners give or were giving CBD to their dogs, and 12% to their cats, most commonly for treating conditions like osteoarthritis (OA), seizures, cancer, or anxiety. From these, 64% found it helps with pain reduction, 50% that it aids with sleep, 49% that it reduces anxiety, and 30% that it reduces convulsions.”
The evidence is generally encouraging for some conditions, particularly pain, but it certainly is nowhere near the level needed to justify this kind of confidence among pet owners. Here are some of the main results reviewed for use of cannabis in various conditions.
The authors also touch on one of the persistent problems with veterinary cannabis products– since they are sold over-the-counter with no meaningful regulation (and often with illegal claims), there is poor quality control. “Some reports have noted inconsistencies in pet CBD supplements that are available in the market, such as misleading or untested claims, violations of good manufacturing practices, lower amounts of CBD than what was stated on the label, and/or THC above the allowed limit (0.3%). Unfortunately, many cannabis products are marketed in the United States with unsubstantiated claims of efficacy.”
As with most studies and reviews, the general conclusion is that the safety profile of non-THC cannabis products is pretty good, though adverse effects do occur. In dogs, there is great variability in the absorption and blood levels of CBD and other relevant compounds with different products and forms, so we still have little idea how much of any given product is safe or useful to give. In cats, the research is even sparser, and since cats appear to be more sensitive to the effects of cannabis-derived compounds (as with most other drugs), the safety and effectiveness of existing products in cats is largely unknown.
Both dogs and cats have show gastrointestinal symptoms (e.g. vomiting and diarrhea0 as well as changes in some laboratory values. Lethargy or sedation and behavioral abnormalities can also occur, especially with products containing THC. It is also recognized that CBD and other compound sin cannabis can build up in fat tissues over time, so even when the short-term risks appear to be low, there is no reliable research identifying what risks might occur with long-term use.
Another narrative review from 2023 focuses on the specific use of cannabis-derived chemicals for treatment of pain.
Miranda-Cortés A, Mota-Rojas D, Crosignani-Outeda N, Casas-Alvarado A, Martínez-Burnes J, Olmos-Hernández A, Mora-Medina P, Verduzco-Mendoza A, Hernández-Ávalos I. The role of cannabinoids in pain modulation in companion animals. Front Vet Sci. 2023 Jan 4;9:1050884. doi: 10.3389/fvets.2022.1050884. PMID: 36686189; PMCID: PMC9848446.
This review mostly addresses the underlying biology of cannabinoids and pain. The few clinical studies mentioned are mostly in dogs with arthritis, and the results are mixed, as discussed in more detail in the previous review. The authors conclude there is some evidence to support use of cannabis-derived chemicals for treatment of both acute and chronic pain, but the evidence is largely extrapolation from lab animal studies (especially rodents), and there is little real-world scientific research in dogs and cats to support this.
Bottom Line
Most other reviews have looked at the same limited set of studies and drawn similar conclusions. What we can currently say about the use of CBD (virtually no evidence related to other compounds in cannabis) is this:
Cannabis is the archetype of a “dirty” drug. It contains hundreds of compounds, most not studied in any depth, and it has effects on many body systems. While this means there is a great potential for cannabis-derived compounds to be useful in many different conditions, it also means the potential for unintended effects and interactions with other drugs is very high unless specific co pounds or subsets of compounds are studied and used individually.
Proponents often talk about the “entourage effect.” This is an idea common in herbal medicine that having multiple compounds in a plant-based remedy is a good thing because they will work in harmony to increase beneficial effects and cancel out each other’s adverse effects. There is no reliable evidence that this phenomenon actually occurs, and it is not very biologically plausible.
The idea originated with the belief that such remedies were purposefully provided to humans by God, and as such were designed to have this benign nature. Only the “unnatural” isolation of individual compounds to use as drugs is responsible for the phenomenon of drug side-effects. This argument is not scientifically credible, and it is far more plausible that mixing multiple compounds leads to more adverse and unintended effects.
Certainly, this is the case with use of cannabis in dogs and cats when THC and CBD are both present in significant amounts. Isolating the CBD reduces these negative effects, so we cannot just assume that using products with multiple compounds and only the THC removed is inherently better than using purified CBD or other cannabis chemicals. Such an entourage effect could occur, but there is not yet compelling evidence for it.
The other important lesson to draw from these recent reviews is that the popularity of cannabis products for dogs and cats is not based on real scientific evidence showing these are safe and effective. This is a fad derived from the popularity of cannabis use in humans, which has origins in ideologies around “natural” medicine, reactions against excessive and largely irrational government prohibitions of cannabis, and factors that have little to do with the actual merits of cannabis as a medicine.
Hopefully, the high level of interest will drive more research, and we will find out what uses it has. I am concerned, however, that the great confidence pet owners already have in cannabis will mean it continues to be profitable to make and sell unregulated and untested products without any motivation for companies doing so to produce meaningful scientific research evidence. Like glucosamine, which has generated billions of dollars for decades despite being almost certainly useless, the cannabis-based supplement market may be just another example of companies seeking profit and consumers seeking panaceas with neither bothering to put in the effort needed to determine what is actually safe and effective treatment for our pets.
The evidence has certainly grown in the ten years since I began discussing the issue. Unfortunately, it is still weak and limited, and the enthusiasm for cannabis has grown much faster than the scientific evidence.
No.
Well, that could easily be the shortest SkeptVet blog post ever, but I guess I can’t really leave it there. For one thing, the answer should really be, “Almost certainly no,” since my level of confidence is high but not absolute. Secondly, it’s the wrong question to be asking, and not one in which I have any interest.
The subject has come up because of some recent publicity around my work with Loyal, a biotechnology company working towards FDA approval for drugs to extend lifespan (the number of years lived) and, more importantly, healthspan (the time lived in good health) in dogs. We recently achieved a pretty exciting milestone on this path, and this has generated a lot of media coverage.
Unfortunately, media coverage of science generally, and veterinary medicine in particular, is often fluffy and ebullient but short on details and nuance. I think a lot of folks may be coming away with the wrong impression about our goals and our work at the company and about what this recent announcement really means. Since SkeptVet readers are hardy enough to tolerate more detailed content, I thought I’d try to set the record a bit straighter here. [Here I will insert the necessary disclaimer that what follows is my understanding and opinion, not the official position of the company I work for.]
I’ve written about aging quite a bit here and in the scientific literature, as well as talking about it for several years at veterinary continuing education meetings (you can check my latest CV for list). My claims about it are simple and, I believe, pretty scientifically sound-
So far, I think, so reasonable. Where thinks get dicey, as always, is what some folks claim is the potential of such interventions, and the extent to which specific approaches are or are not yet “proven” to affect aging and health. Again, my claims here are pretty simple, and I think reasonable-
Even these require further research to validate and clarify the specific approaches and the effects on lifespan and aging-associated health problems.
With that as the context, what have we achieved at Loyal and what does it really mean?
We have chosen to pursue FDA approval for prescription medications, rather than whipping up an “anti-aging” supplement to sell with minimal oversight and evidence, because we believe this process better ensures the final product is safe and effective. FDA approval is a pretty high bar, but it is by no means requires the highest possible level of evidence. As a refresher, here is the pyramid of evidence I have harped on for years-

The best evidence for any medical intervention is ultimately a solid foundation in well-understood basic science (i.e. biologic plausibility) combined with multiple high-quality clinical trials conducted by multiple investigators with different biases and agendas. This, sadly, is a level of evidence virtually never available in veterinary medicine due to the time, expense, and logistically challenges in producing it.
The best we can usually hope for is biologic plausibility demonstrated by decent pre-clinical evidence and then one or two moderate-quality clinical trials with decent bias-control mechanisms. Even this is more than the vast majority of therapies in current use in veterinary medicine have, but if we sit on our hands and wait for perfect evidence, we won’t have any tools to help our patients.
I have always said that we should choose the best therapy we can based on the best available evidence. That may be no more than a handful of anecdotes (sadly), but that can be appropriate if the need is great enough, we give the client sufficient honest information to understand the risks and uncertainties, and we proportion our confidence in the treatment to the level of evidence so that we can abandon treatments that are unsafe or ineffective when new evidence comes along.
In the case of regular FDA approval, there is a requirement for strong evidence to support biologic plausibility (a plausible mechanism of action, research evidence showing the drug is present in the body and acting on the physiologic pathways it is supposed to act on, etc.), safety (including testing in individuals of the species the drug will be used on at multiple doses, including some that are higher than the actually intended clinical dose), appropriate manufacturing methods, and no significant negative impact on the environment or human food safety.
There is also a requirement to prove clinical effectiveness– that the drug actually does what it is meant to do in animal patients. This last criterion usually requires a well-designed and properly conducted field trial, meaning a clinical trial in real-world patients. While this is, again, not the best evidence one could possibly ask for, it is strong evidence and far better than most veterinary therapies ever achieve.
The FDA also allows a slightly different pathway for what is called “conditional approval.” In situations where there is a serious health problem for which no proven effective treatment exists, a new treatment can sometimes be conditionally approved to be used in patients before completion of this field trial. All of the other criteria must still be met as usual, including demonstration of safety, but effectiveness can be substantiated by showing “reasonable expectations of effectiveness” through evidence other than a full clinical field trial. Even this is only allowed if conducting a field trial would be so complex and time-consuming that it would significantly delay the availability of the drug to patients who, again, have a serious health problem with no currently available approved treatments.
The field trial must still be done, but the drug can be made available temporarily (for one year at a time up to a total of five years). This is intended as a compromise between the need for strong evidence to support efficacy and the need for new treatments to be made available to patients with serious health problems as quickly as possible.
There are several conditionally approved therapies on the market now, including-
So what does all of this have to do with our work at Loyal? Well, we recently received a notice from the FDA indicating that the agency accepted the evidence we submitted for one of our products, called LOY-001, as sufficient to meet the standard for a reasonable expectation of efficacy. Let’s start with what this doesn’t mean-
With that clarification, I will address some of the questions and concerns I have heard since the announcement.
To begin with, some folks feel that the conditional approval pathway is insufficient to demonstrate effectiveness and that no drug should be used until it achieves full approval after a field trial. That’s a perfectly reasonable position, and I won’t try to argue anyone out of it. I will point out, though, that the purpose of having a conditional approval process is to acknowledge that delaying the availability of new treatments while a field trial is completed, especially one that will take a long time, does have a cost as well as a benefit. While the final evidence is stronger, and while we may be glad we waited if the field trial doesn’t confirm the expectation of effectiveness, patients are going without treatment while we wait.
Aging is arguably responsible for the vast majority of the disability, disease, and death we see in senior dogs, and there are no approved or well-validated treatments currently available to target this major cause of suffering, so it certainly represents an unmet need. The fact that we have always accepted it as inevitable and immutable doesn’t mean there is no urgency to developing treatments for it, only that we aren’t yet accustomed to thinking about the harms of aging the way we think about the harms from cancer, chronic kidney disease, or other health problems in our pets and patients.
Obviously, any clinical trial evaluating the effect of a drug on lifespan is going to be complex and take a long time. We are planning several such trials. The first, for a different product, is starting this month and will involve 1,000 dogs studied over 4-5 years. This is probably the largest clinical trial ever done in veterinary medicine, so it certainly counts as complex and prolonged. A field trial of LOY-001 would likely be very similar.
If LOY-001, or any other drug targeting aging, achieves conditional approval, it will have met the same standards of evidence for safety as any fully approved drug. Vets and dog owners will then have to decide whether the potential benefits outweigh the uncertainties inherent in the reasonable expectation of effectiveness standard and whether they want to use the drug right away, wait until a field trial is complete and it is fully approved, wait until the drug has been in use for some period of time after approval, or whatever other standard of evidence they feel is appropriate. That is the same decision we all must make for any new treatment that becomes available, and there is no absolute or universally “right” or “wrong” choice.
Some readers have expressed concern that I am helping to work towards conditional approval for this drug while having been critical of other treatments, both conventional and alternative, based on claims or uses for these without sufficient evidence. This seems inconsistent to some folks. I don’t believe that is the case, and I think a close reading of my critiques of many different therapies will show that I do not argue absolutely against the use of anything unless there is either clear evidence that the risk outweighs the benefits. I frequently point out that using even therapies with minimal supporting evidence is fair if, as I said earlier, the need is sufficient, there is informed consent, and we don’t make claims with unjustifiable confidence.
In the case of any conditionally approved product, including those that may become available from Loyal, I believe the risks and benefits of their use should be weighed in the context of the uncertainty and claims should be proportional to the strength of the evidence. If LOY-001 or another Loyal product becomes available under the conditional approval pathway, I will apply this same standard. As of now, I am not making any claims since there is no approved product to make them for.
I have also been asked why, if there is no drug actually available, this milestone matters at all. The answer to that has to do with the issue of how aging is approached in veterinary and human medicine.
We have traditionally played a game of whack-a-mole with age-associated health problems—waiting for them to appear and then treating them as best we can. Since aging has been considered inevitable and just a fact of the universe, we haven’t thought much about it in terms of prevention or of treating the underlying causal mechanisms of age-associated disease. This has included a reluctance to consider aging a treatable problem for which drugs could be developed and approved. The FDA acceptance of our evidence for reasonable expectations of effectiveness is the first time, as far as we can tell, that the FDA or any other health regulator has accepted the idea that a treatment could be approved for extending lifespan or mitigating the consequences of aging by targeting the mechanisms of aging directly.
This opens up the possibility of an entire new field of medicine and a proactive, preventative approach to aging. Whether or not LOY-001 or any other specific drug achieves approval, this is a significant milestone in the effort to change how we approach aging and age-associated health problems. For once, veterinary medicine is leading rather than following human medicine!
Finally, there is the question of my own bias with regard to this and other products produced by Loyal because I am an employee of the company. The question is not whether or not I have a bias, because of course I do! I have a financial interest in the success of the company, and while I believe my ethics would prevent me from saying anything misleading or untruthful about the company or our products, financial bias is a reality, and it is fair to acknowledge the potential subtle and unconscious influences this may have on anyone.
As I have explained many times before, though, I think the more interesting and important source of bias is ideological and institutional. I wouldn’t work for Loyal if I didn’t feel like the values and goals and scientific work being done there didn’t already align with my own views and values. I tend to agree with the approach to aging and the way we are going about our work not because I get paid by the company but because I chose to work for them in the first place because of this alignment!
Does that mean anything I say about the company or our products is meaningless or should be dismissed due to my bias? Well, that’s up to each reader to decide for themselves. What I will say is that, in an ideal world, no claim about a medical intervention should ever be accepted entirely on the basis of the opinions of any individual, including me. We should all review the objective evidence critically and make our own decisions. If our products achieve conditional or full approval, the evidence will all be publicly available for people to use in making up their own minds.
That said, we can’t all be experts on every subject, and we don’t always have the time or skills to evaluate every claim effectively on our own. When I have questions about infectious diseases, I give great weight to the opinions of trusted experts who I know have an evidence-based approach and the expertise to make critical judgement about this area (e.g. Dr. Weese). I do the same in other areas, relying on the expertise of nutritionists (e.g. Dr. Larsen, Dr. Weeth, Dr. Villaverde), cardiologists (e.g. Dr. Rishniw), and so on. I balance independent critical thinking with a recognition of the inevitable limitations of my own knowledge and capacity, and I rely on others to help inform my understanding of specific topics.
We all have to do this since we cannot know everything about everything. The biggest challenge is identifying reliable sources and striking a balance that doesn’t fall into the traps of overconfident independence on one end or blind following of equally imperfect humans on the other. How people choose to regard my opinions and evaluation of any subject, including aging therapies, will be a decision of this sort.
I first began writing about potential medical uses for cannabis products in pets ten years ago. AT the time, there was weak evidence for a few uses in humans, and almost no research evidence in dogs or cats. Since then, I have covered the topic frequently, and new evidence has appeared regularly. This evidence has been mixed, with some studies suggesting benefits and others not. Generally, the safety data has suggested minimal risk, though a recent recommendation to lower the maximum daily dose of CBD in humans reflects the fact that there is much we still don’t know about the potential consequences of long-term use of cannabis-based compounds.
It is currently vogue to use CBD for a wide-range of problems in dogs and cats, and there is little to no evidence to support most of these uses. The most common use, and that with the best evidence, is for pain. However, even in humans there is controversy about how effective CBD and other cannabis-based compounds are for pain. A recent systematic review found that,
“Studies in this field have unclear or high risk of bias, and outcomes had GRADE rating of low- or very low-quality evidence. We have little confidence in the estimates of effect. The evidence neither supports nor refutes claims of efficacy and safety for cannabinoids, cannabis, or CBM in the management of pain.”
A similar systematic review was recently published for the use of CBD in treatment of arthritis in dogs.
Patikorn C, Nerapusee O, Soontornvipart K, Lawonyawut K, Musikpodok K, Waleethanaphan K, Anantachoti P. Efficacy and safety of cannabidiol for the treatment of canine osteoarthritis: a systematic review and meta-analysis of animal intervention studies. Front Vet Sci. 2023 Sep 15;10:1248417.
As a refresher, a systematic review is the highest level of research evidence available for most questions. It involves the explicit and formal finding and analysis of controlled research studies on a given topic. Such reviews are not perfect nor free from bias, and they are less useful the less roust the primary research evidence is, but they give the best overview of an issue based on the highest quality evidence currently available.
The conclusion of this review is typical of many in veterinary medicine:
“Five articles were included, which investigated the effects of CBD in 117 dogs with OA. All studies were rated as having a high risk of bias.
CBD is considered safe for treating canine OA. CBD may reduce pain scores, but the evidence is very uncertain to conclude its clinical efficacy. High-quality clinical trials are needed to further evaluate the roles of CBD in canine OA.”
There have been relatively few studies involving few patients and all with significant methodological risk of bias. From this kind of evidence base, the best we can safely conclude is that CBD might have some benefits for dogs in pain and probably doesn’t have any acute risks.
That is sufficient to consider adding it in as a treatment for dogs with arthritis not sufficiently controlled by other treatments, but NOT to use it as a first-line treatment or a substitute for treatments with better evidence for efficacy (such as non-steroidal anti-inflammatory drugs).




